

Construction and validation of a nomogram for predicting overall survival in stage IV non-small cell lung cancer treated with epidermal growth factor receptor tyrosine kinase inhibitors
- PMID: 40809246
- PMCID: PMC12340277
- DOI: 10.21037/jtd-2024-2112
Construction and validation of a nomogram for predicting overall survival in stage IV non-small cell lung cancer treated with epidermal growth factor receptor tyrosine kinase inhibitors
Abstract
Background: Despite the widespread adoption of epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) as the primary therapeutic strategy for EGFR mutated non-small cell lung cancer (NSCLC), the general survival probabilities for patients in stage IV are still limited. The objective of this research was to create a nomogram that forecasts overall survival (OS) in patients with advanced NSCLC undergoing EGFR-TKI treatment.
Methods: A group of 461 patients with advanced EGFR-mutant NSCLC was recruited and randomly divided into training and validation sets in a ratio of 7:3. The predictive nomogram was constructed after identifying independent prognostic factors within the training group by applying the Cox regression analysis. The nomogram was evaluated by R software, with assessments including decision curve analyses, receiver operating characteristic curves, and calibration curves.
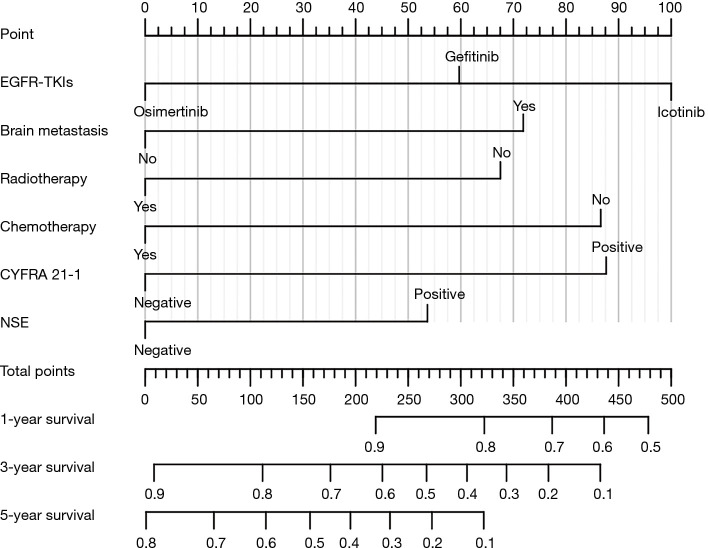
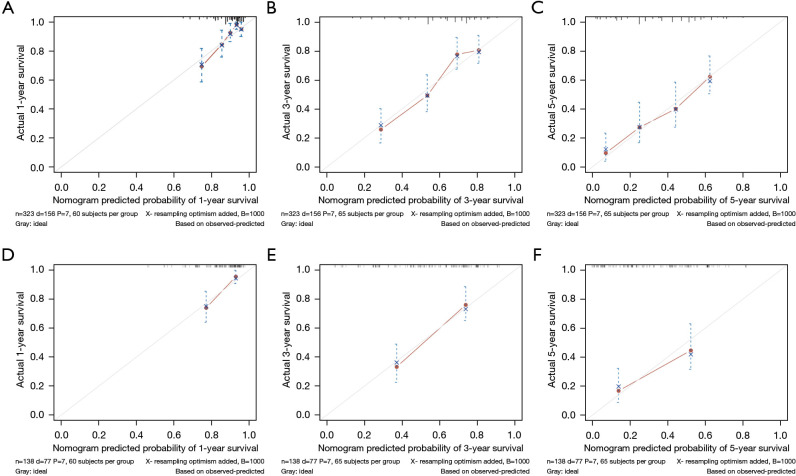
Results: Multivariate Cox regression identified brain metastasis, neuron-specific enolase (NSE), cytokeratin fragment 19 (CYFRA 21-1), EGFR-TKIs, radiotherapy, and chemotherapy as independent prognostic factors. The nomogram was constructed based on these prognostic factors. The C-index was 0.713 in both the training and validation cohorts, with calibration curves demonstrating strong concordance between predicted and actual outcomes. The area under the receiver operating characteristic curve demonstrated robust predictive accuracy, with values of 0.771, 0.772, and 0.768 at 1, 3, and 5 years in the training cohort, and 0.802, 0.761, and 0.722 in the validation cohort. Decision curve analysis (DCA) confirmed the strong clinical applicability of the nomogram. Based on the nomogram scores, patients were stratified into high- and low-risk groups, with OS markedly increased in the latter group over the former (P<0.001).
Conclusions: The nomogram was created using clinical features to forecast OS in stage IV NSCLC patients with EGFR mutations undergoing EGFR-TKI therapy.
Keywords: Epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs); nomogram; non-small cell lung cancer (NSCLC); overall survival (OS); stage IV.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2024-2112/coif). The authors have no conflicts of interest to declare.
Figures





Similar articles
-
Clinical diagnostic and prognostic value of homocysteine combined with hemoglobin [f (Hcy-Hb)] in cardio-renal syndrome caused by primary acute myocardial infarction.J Transl Med. 2025 Jul 23;23(1):813. doi: 10.1186/s12967-025-06512-4. J Transl Med. 2025. PMID: 40702542 Free PMC article.
-
Construction of a clinical prediction model for overall survival and cancer-specific survival in malignant phyllode tumor of the breast based on the SEER database.Discov Oncol. 2025 Jul 1;16(1):1200. doi: 10.1007/s12672-025-03024-x. Discov Oncol. 2025. PMID: 40591139 Free PMC article.
-
Construction and validation of a novel prognostic nomogram for predicting overall survival in lung adenocarcinoma patients with different patterns of metastasis.J Cancer Res Clin Oncol. 2023 Nov;149(16):15039-15053. doi: 10.1007/s00432-023-05288-8. Epub 2023 Aug 23. J Cancer Res Clin Oncol. 2023. PMID: 37612389 Free PMC article.
-
Epidermal growth factor receptor tyrosine kinase (EGFR-TK) mutation testing in adults with locally advanced or metastatic non-small cell lung cancer: a systematic review and cost-effectiveness analysis.Health Technol Assess. 2014 May;18(32):1-166. doi: 10.3310/hta18320. Health Technol Assess. 2014. PMID: 24827857 Free PMC article.
-
Adjuvant epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) for the treatment of people with resected stage I to III non-small-cell lung cancer and EGFR mutation.Cochrane Database Syst Rev. 2025 May 27;5(5):CD015140. doi: 10.1002/14651858.CD015140.pub2. Cochrane Database Syst Rev. 2025. PMID: 40421698 Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous