

Compared with assessment via endoscopic examination, assessment through the examination of resected regional lymph nodes can significantly reduce the mortality rate of lung cancer patients: a retrospective study of 222,563 participants from the SEER database
- PMID: 40809247
- PMCID: PMC12340294
- DOI: 10.21037/jtd-2025-821
Compared with assessment via endoscopic examination, assessment through the examination of resected regional lymph nodes can significantly reduce the mortality rate of lung cancer patients: a retrospective study of 222,563 participants from the SEER database
Abstract
Background: Lymph node assessment is essential for determining treatment and evaluating the surgical scope in patients with lung cancer, thus significantly impacting survival prognosis. Surgical resection and endoscopic biopsy are the primary methods for obtaining lymph node samples, yet it remains controversial to determine which approach can provide greater benefit. This study aims to analyze the prognosis and survival outcomes of lung cancer patients who undergo assessment through the examination of resected regional lymph nodes, assessment via endoscopic examination, or assessment based on imaging modalities.
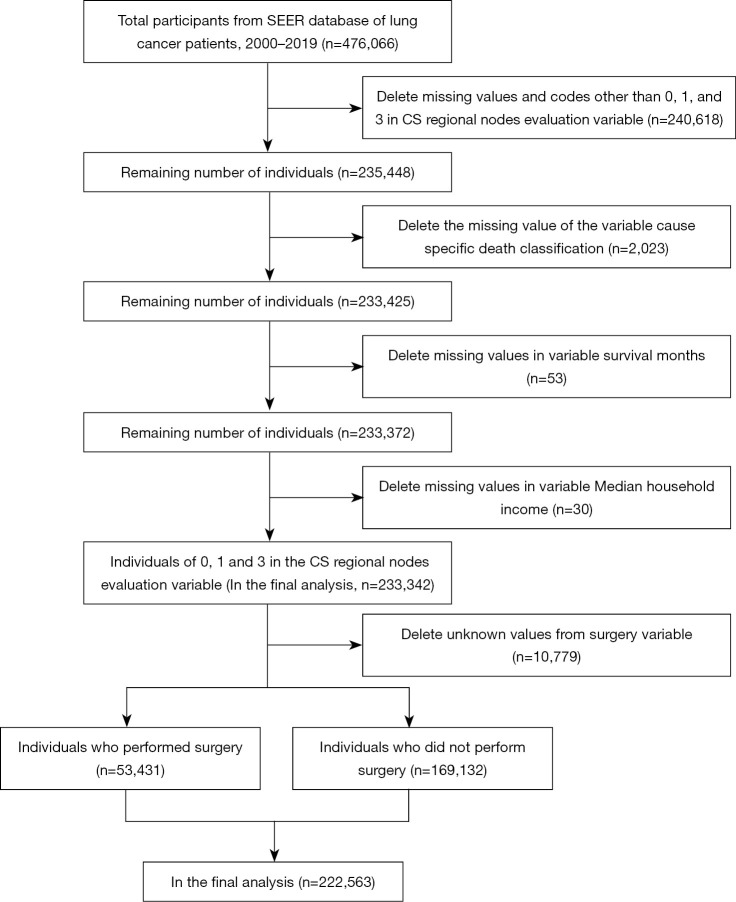
Methods: Data from the Surveillance, Epidemiology, and End Results (SEER) database, comprising 222,563 participants, were analyzed. The outcome variables were overall survival (OS) and lung cancer-specific mortality, while the primary variable was the method of lymph node assessment. Life table, Kaplan-Meier survival, and Cox proportional hazards analyses were conducted, with log-rank Mantel-Cox, Breslow generalized Wilcoxon, and Tarone-Ware tests being applied for intergroup comparisons.
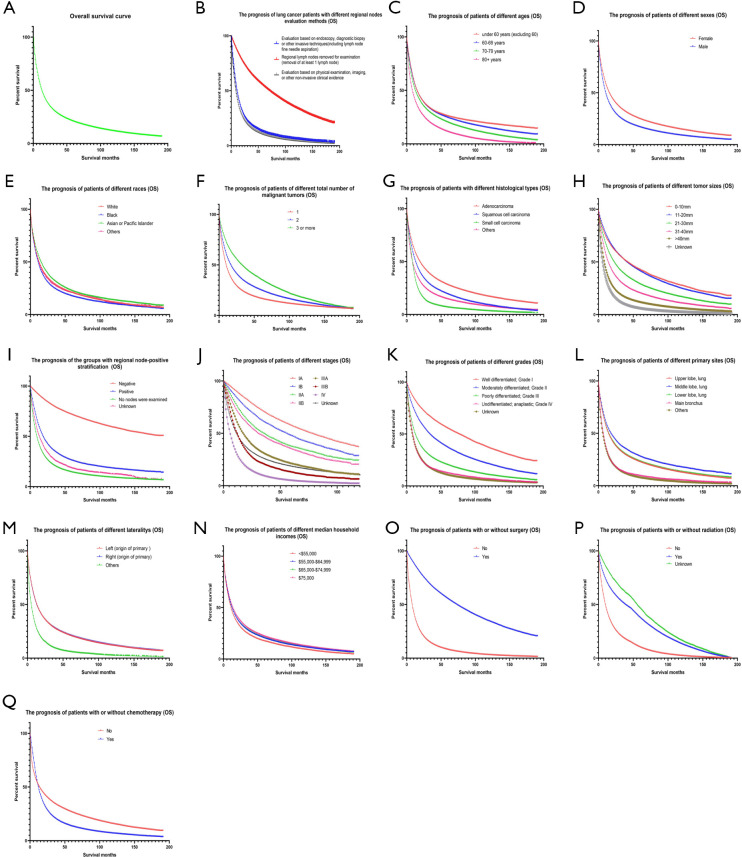
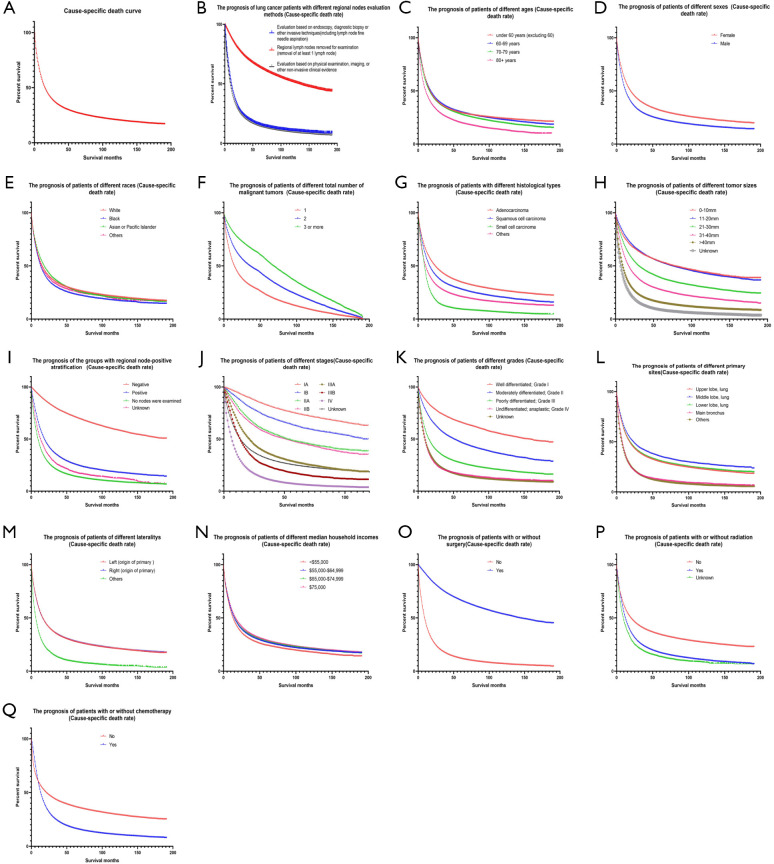
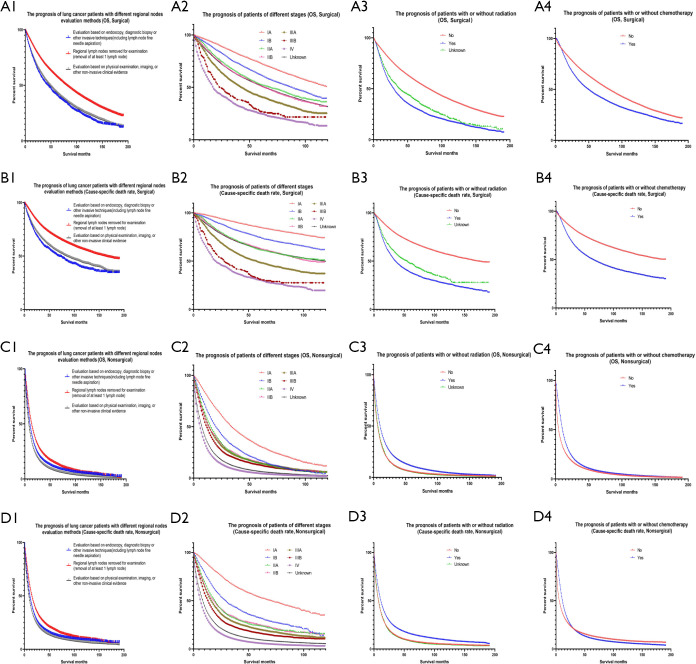
Results: Compared to endoscopic biopsy, lymph node resection examination reduced the risk of death by 15.7% (P<0.001) and the lung cancer-specific mortality rate by 15.5% (P<0.001). Lung cancer patients who underwent regional lymph node resection examination had higher OS rates at 1, 2, 3, 5, 10, and 15 years by 44%, 49%, 47%, 42%, 28%, and 20%, respectively, compared to those who underwent endoscopic biopsy. Additionally, their cancer-specific survival rates were higher at the corresponding time points by 13%, 16%, 17%, 17%, 18%, and 13%, respectively. The mean OS period for patients who underwent endoscopic lymph node biopsy was 25.071 months, whereas for lung cancer patients who underwent regional lymph node resection examination, the average OS was 87.403 months.
Conclusions: In patients with lung cancer, lymph node resection examination significantly reduces mortality and improves survival as compared to endoscopic biopsy.
Keywords: Lung cancer; Surveillance, Epidemiology, and End Results (SEER); lymph node; survival.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2025-821/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
[Relationship between primary tumor lymph node indicators and prognosis and treatment response in colorectal cancer patients with lung metastases].Zhonghua Yi Xue Za Zhi. 2025 Aug 5;105(29):2491-2499. doi: 10.3760/cma.j.cn112137-20250324-00724. Zhonghua Yi Xue Za Zhi. 2025. PMID: 40764092 Chinese.
-
Lymphadenectomy or sentinel node biopsy for the management of endometrial cancer.Cochrane Database Syst Rev. 2025 Jun 10;6(6):CD015786. doi: 10.1002/14651858.CD015786.pub2. Cochrane Database Syst Rev. 2025. PMID: 40492478 Review.
-
[Application research of endoscopic-laparoscopic regional gastric resection combined with sentinel lymph node basin dissection in patients with early gastric cancer].Zhonghua Wai Ke Za Zhi. 2025 Jul 1;63(7):587-596. doi: 10.3760/cma.j.cn112139-20250117-00034. Zhonghua Wai Ke Za Zhi. 2025. PMID: 40443334 Chinese.
-
Sublobar resection is non-inferior to lobectomy in octogenarians and older with stage Ia non‑small cell lung cancer.Transl Cancer Res. 2025 May 30;14(5):2966-2980. doi: 10.21037/tcr-2024-2575. Epub 2025 May 14. Transl Cancer Res. 2025. PMID: 40530121 Free PMC article.
-
Systemic treatments for metastatic cutaneous melanoma.Cochrane Database Syst Rev. 2018 Feb 6;2(2):CD011123. doi: 10.1002/14651858.CD011123.pub2. Cochrane Database Syst Rev. 2018. PMID: 29405038 Free PMC article.
References
LinkOut - more resources
Full Text Sources