

Key risk factors for mortality after pneumonectomy for lung cancer: insights from a large single-center cohort study
- PMID: 40809274
- PMCID: PMC12340288
- DOI: 10.21037/jtd-2024-2204
Key risk factors for mortality after pneumonectomy for lung cancer: insights from a large single-center cohort study
Abstract
Background: Surgery remains the most effective treatment for patients with non-small cell lung cancer (NSCLC). However, pneumonectomy is usually associated with high mortality and morbidity rates. Defining post-operative death after such extensive procedures remains controversial. This study aimed to assess the 30- and 90-day post-pneumonectomy mortality rates. The secondary aim was to identify the most critical factors determining early post-pneumonectomy mortality.
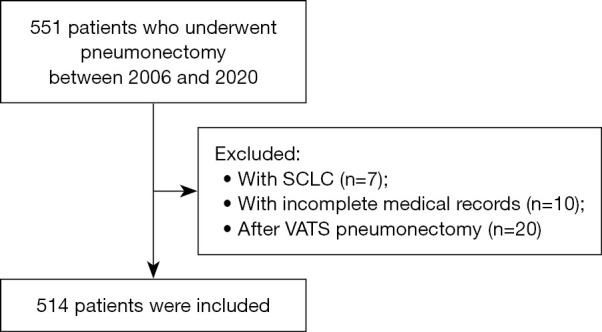
Methods: This retrospective, single-institution cohort study was conducted at a high-volume center and included a large group of 514 patients who underwent pneumonectomy for NSCLC from 2006 to 2020. Our analysis considered patient comorbidities, staging, surgical techniques, neoadjuvant chemotherapy, and major complications, and examined their associations with 30- and 90-day mortality rates. We initially performed a univariable Cox regression analysis, followed by multivariable analyses, including variables with P<0.1.
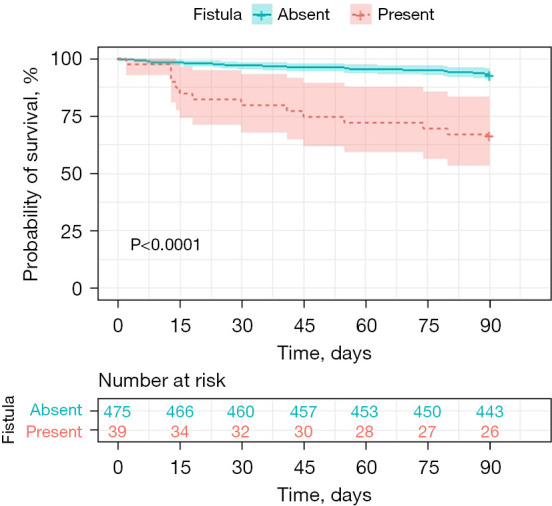
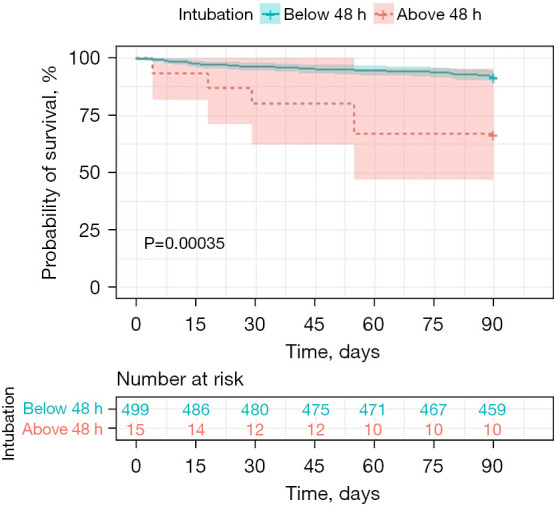
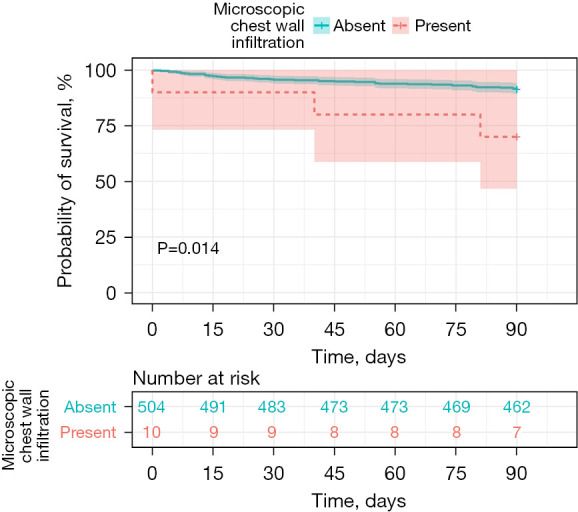
Results: The 30- and 90-day mortality was equal to 4.3% and 9.1%, respectively. For 30-day mortality, statistically significant factors included the occurrence of a bronchopleural fistula (BPF) [hazard ratio (HR) =5.128; 95% confidence interval (CI): 2.009-13.087; P<0.001], positive bronchial resection margin (HR =7.917; 95% CI: 2.61-24.01; P<0.001) and the prolonged intubation (>48 hours) (HR =3.822; 95% CI: 1.06-13.785; P=0.041). For the 90-day mortality, the presence of the BPF (HR =5.284; 95% CI: 2.706-10.318; P<0.001), positive bronchial resection margin (HR =3.528; 95% CI: 1.370-9.083; P=0.009), chest wall infiltration (HR =3.770; 95% CI: 1.121-12.676; P=0.03), and prolonged intubation (>48 hours) (HR =2.912; 95% CI: 1.102-7.649; P=0.03) were the statistically significant risk factors.
Conclusions: A 90-day follow-up period should be considered when assessing short-term mortality rates after major pulmonary resections. Monitoring long-term mortality is important, as the mortality rate in our group doubled after 3 months. BPF, prolonged intubation, chest wall infiltration, and positive bronchial resection margin significantly increase the risk of 30- and 90-day mortality rates.
Keywords: 30-day mortality; 90-day mortality; bronchopleural fistula (BPF); non-small cell lung cancer (NSCLC); pneumonectomy.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2024-2204/coif). Mikołaj Kamiński reports that he has received support for conference participation from the following companies: Medac, Berlin-Chemie Menarini, Boehringer Ingelheim, and Eli Lilly. The other authors have no conflicts of interest to declare.
Figures


Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26;483(9):1680-95. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
-
[Guidelines for the prevention and management of bronchial asthma (2024 edition)].Zhonghua Jie He He Hu Xi Za Zhi. 2025 Mar 12;48(3):208-248. doi: 10.3760/cma.j.cn112147-20241013-00601. Zhonghua Jie He He Hu Xi Za Zhi. 2025. PMID: 40050074 Chinese.
-
Systemic treatments for metastatic cutaneous melanoma.Cochrane Database Syst Rev. 2018 Feb 6;2(2):CD011123. doi: 10.1002/14651858.CD011123.pub2. Cochrane Database Syst Rev. 2018. PMID: 29405038 Free PMC article.
References
LinkOut - more resources
Full Text Sources