

Case Reports
doi: 10.1016/j.radcr.2025.06.083.
eCollection 2025 Oct.
A radiological case series of diverse vaginal cuff lesions
Affiliations
- PMID: 40809309
- PMCID: PMC12344950
- DOI: 10.1016/j.radcr.2025.06.083
Item in Clipboard
Case Reports
A radiological case series of diverse vaginal cuff lesions
Radiol Case Rep.
.
Abstract
This case series explores 4 unique presentations of vaginal cuff lesions, highlighting their diverse etiologies and imaging characteristics. The cases include a vaginal cuff meshoma, benign vaginal cuff cystic lesions, and metastatic endometroid adenocarcinoma. The series emphasizes the importance of a multifaceted approach utilizing patient history, clinical examination, and various imaging modalities (transvaginal ultrasound, MRI, PET-CT) for accurate diagnosis and optimal patient management.
Keywords: Gartner duct cyst; Inclusion cyst; Meshoma; Metastases; Vaginal cuff lesions.
© 2025 The Authors.
Figures
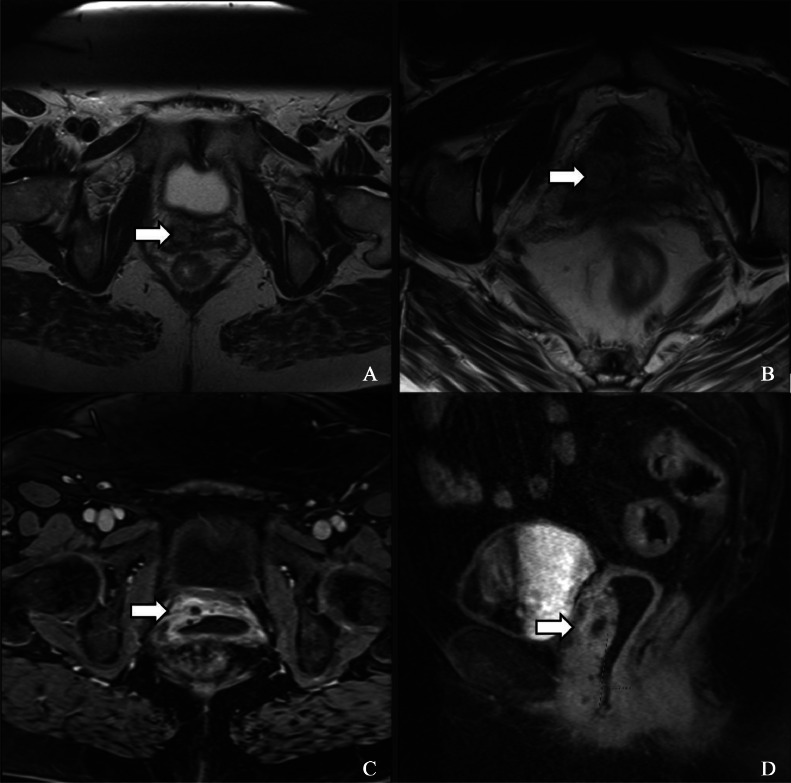
(A and B) T2-weighted MRI image showing mesh embedded in the anterior vaginal wall (white arrow). (C and D) MRI postcontrast image showing a peripheral enhancing soft tissue mass seen along the anterior vaginal cuff in the paramedian location (white arrow).
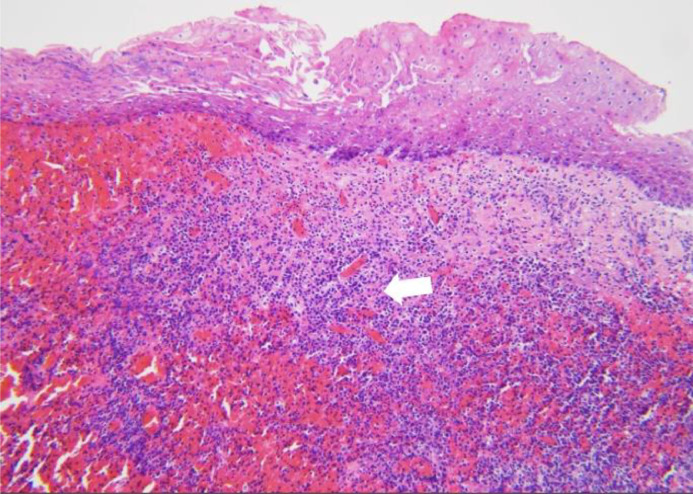
Histopathology section of the attached tissue to excised vaginal mesh demonstrating squamous mucosa with submucosal hemorrhage, acute and chronic inflammation (marked with white arrow), and necrosis (H&E stain, 100x magnification).
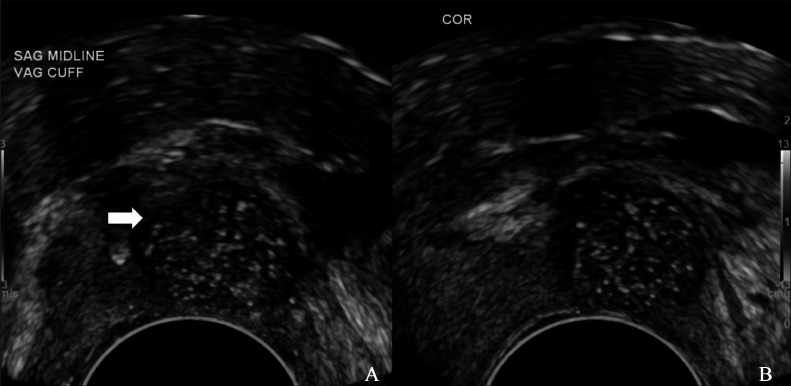
Sagittal (A) and coronal (B) transvaginal ultrasound showing a predominantly hypoechoic lesion (marked with white arrow), measuring 1.6 × 1.3 × 1.4 cm, with multiple punctate hyperechoic foci within.
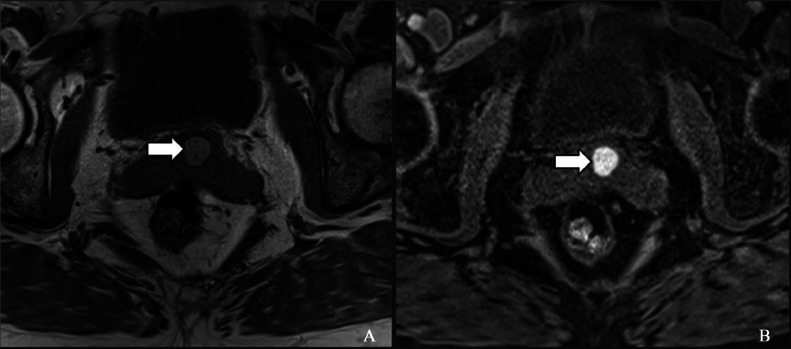
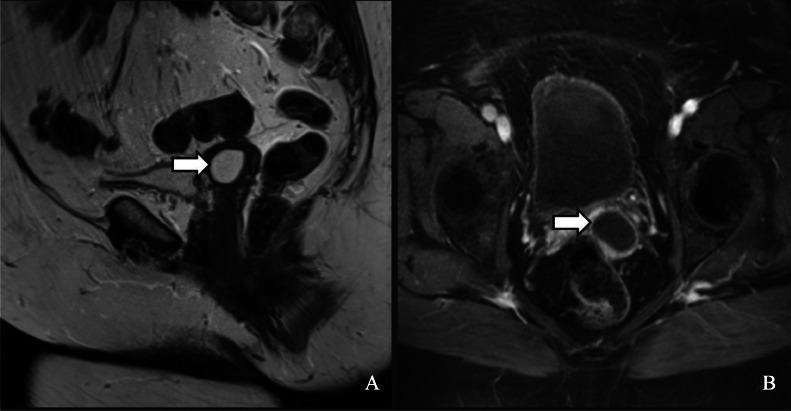
MRI T1 weighted noncontrast nonfat suppressed (A) and fat-suppressed (B) images showing the well-defined anterior vaginal wall inclusion cyst ( marked with white arrows). It appears hyperintense in both images and is not suppressed on fat-suppressed imaging.
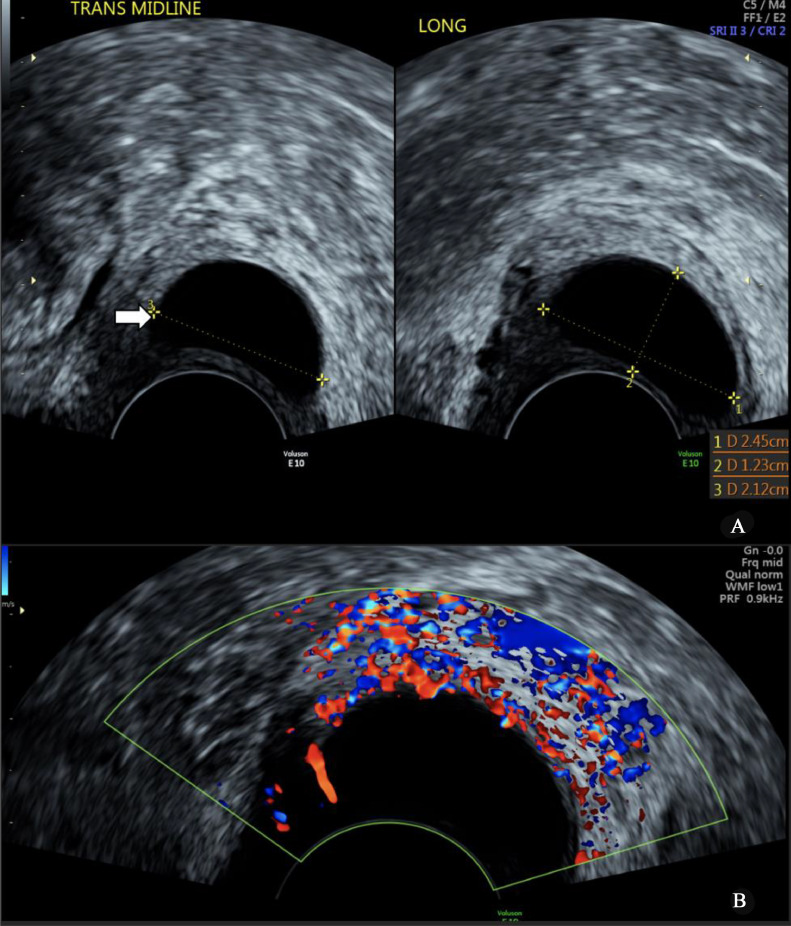
Transvaginal ultrasound image (A) displaying a well-defined anechoic cyst (white arrow) with peripheral vascularity within the vaginal cuff (B).
T2-weighted MRI image (A) showing a hyperintense lesion (white arrow) with mild peripheral enhancement (white arrow) on T1 contrast MRI image (B).
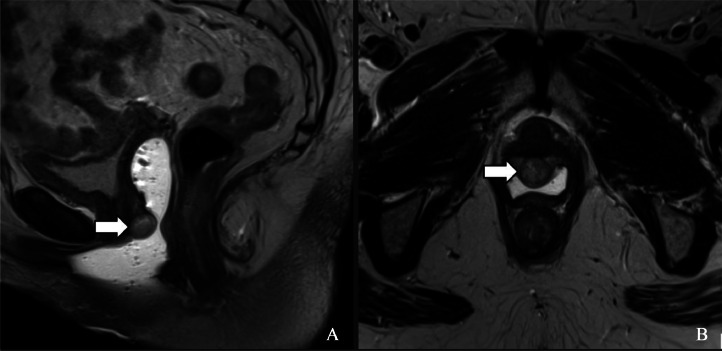
Sagittal (A) and axial (B) T2 weighted MRI images showing the new metastatic vaginal lesion (white arrows). It is a well-defined heterogenous lesion along the anterior wall of the vaginal cuff, just posterior to the urethral meatus.

Axial MRI images, showing diffusion restriction with hyperintensity on DWI (A) and hypointensity on ADC image (B).
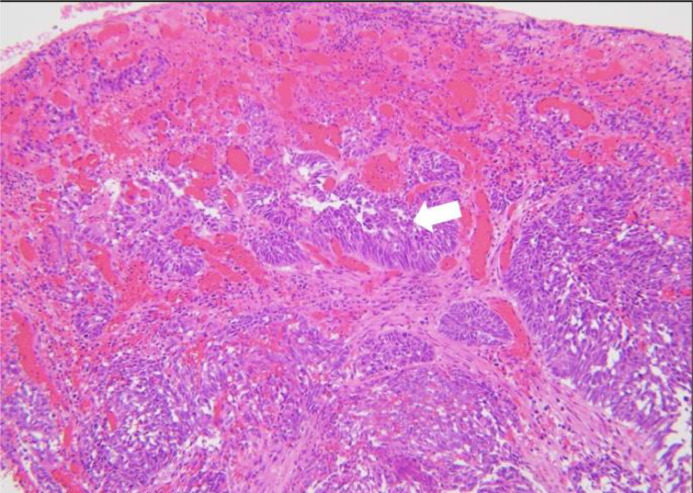
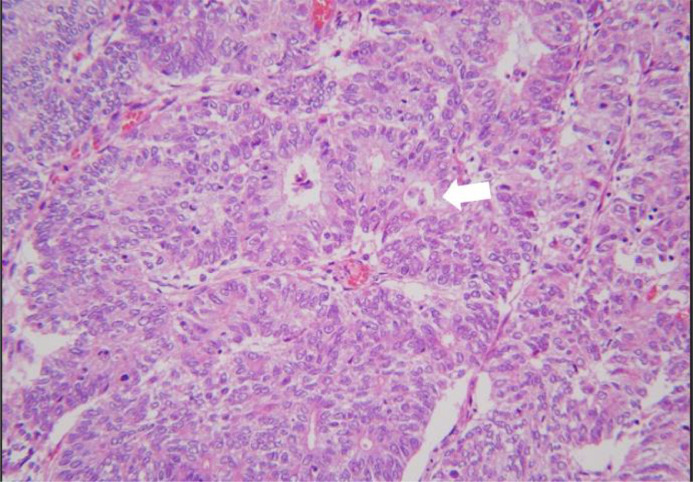
Histopathological image showing infiltrating malignant glands (marked with white arrow) throughout the vaginal mucosa. The malignant glands are morphologically identical to those observed in the prior hysterectomy specimen, which showed endometrioid adenocarcinoma. The findings indicate metastatic involvement of the vagina by the patient's primary endometrial cancer. (H&E stain, 100x magnification).
Histology of hysterectomy specimen showing infiltrating malignant glands (marked with white arrow) in Endometrial carcinoma, endometrioid type, FIGO Grade 3 with residual 20% myometrial invasion (H&E stain, 200× magnification).
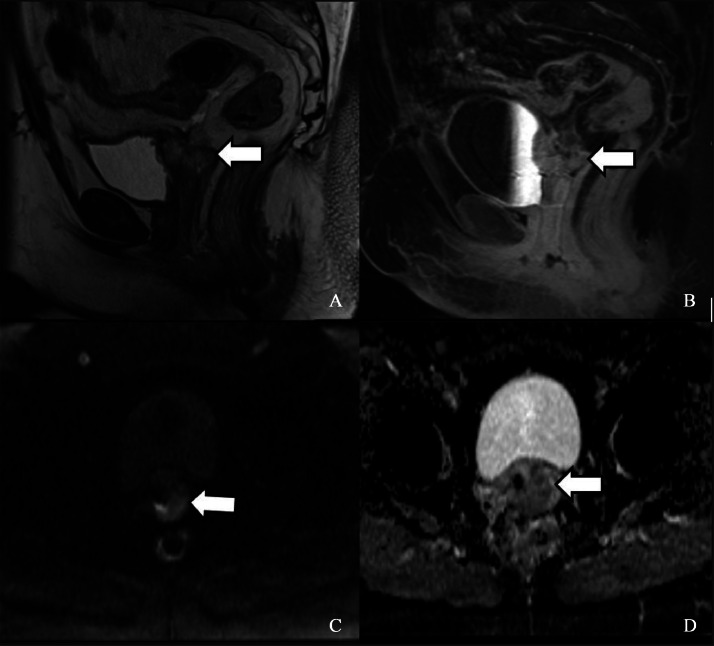
MRI Pelvis images showing intermediate signal heterogenous nodular thickening involving top of vaginal cuff on T2W sequence (A) and contrast enhancement is seen in sagittal T1 contrast image (B). Axial MRI images showing mild diffusion restriction with mild hyperintensity on DWI (C) and hypointensity on ADC sequence (D) (marked with white arrow).

FDG PET Coronal (A) and Axial (B) images show intense FDG avidity in vaginal cuff lesions (marked with white arrow).
Similar articles
-
Symptomatic Vaginal Masses Mimicking Prolapse: Varied Clinical Course, Diagnosis and Their Management.J Obstet Gynaecol India. 2025 Apr;75(Suppl 1):9-13. doi: 10.1007/s13224-024-01964-y. Epub 2024 Mar 25. J Obstet Gynaecol India. 2025. PMID: 40390928
-
Imaging modalities for characterising focal pancreatic lesions.Cochrane Database Syst Rev. 2017 Apr 17;4(4):CD010213. doi: 10.1002/14651858.CD010213.pub2. Cochrane Database Syst Rev. 2017. PMID: 28415140 Free PMC article.
-
Imaging of indeterminate pancreatic cystic lesions: a systematic review.Pancreatology. 2013 Jul-Aug;13(4):436-42. doi: 10.1016/j.pan.2013.05.007. Epub 2013 Jun 4. Pancreatology. 2013. PMID: 23890144
-
123I-MIBG scintigraphy and 18F-FDG-PET imaging for diagnosing neuroblastoma.Cochrane Database Syst Rev. 2015 Sep 29;2015(9):CD009263. doi: 10.1002/14651858.CD009263.pub2. Cochrane Database Syst Rev. 2015. PMID: 26417712 Free PMC article.
-
Renal hydatid cyst mimicking malignancy: a case report.Int J Surg Case Rep. 2025 Jul;132:111506. doi: 10.1016/j.ijscr.2025.111506. Epub 2025 Jun 13. Int J Surg Case Rep. 2025. PMID: 40517679 Free PMC article.
References
-
- Stein M.W., Grishina A., Shaw R.J., Roberts J.H., Ricci Z.J., Adachi A., et al. Gray-scale and color doppler sonographic features of the vaginal cuff and cervical remnant after hysterectomy. AJR Am J Roentgenol. 2006;187(5):1372–1376. - PubMed
-
- Visco A.G., Weidner A.C., Barber M.D., Myers E.R., Cundiff G.W., Bump R.C., et al. Vaginal mesh erosion after abdominal sacral colpopexy. Am J Obstet Gynecol. 2001;184(3):297–302. - PubMed
-
- Amid P.K. Radiologic images of meshoma: a new phenomenon causing chronic pain after prosthetic repair of abdominal wall hernias. Arch Surg. 2004;139(12):1297–1298. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
