

Emergency risk stratification using the TyG index: a multi-center cohort study on nonlinear association with 28-day mortality among critically ill patients transferred from the ED to the ICU
- PMID: 40809413
- PMCID: PMC12343646
- DOI: 10.3389/fmed.2025.1605843
Emergency risk stratification using the TyG index: a multi-center cohort study on nonlinear association with 28-day mortality among critically ill patients transferred from the ED to the ICU
Abstract
Background: In the emergency department (ED), rapid risk stratification of critically ill patients is essential for timely intervention. The triglyceride-glucose (TyG) index, a simple marker of insulin resistance, may aid in early mortality prediction, but its utility in ED-to-ICU patients remains unexplored.
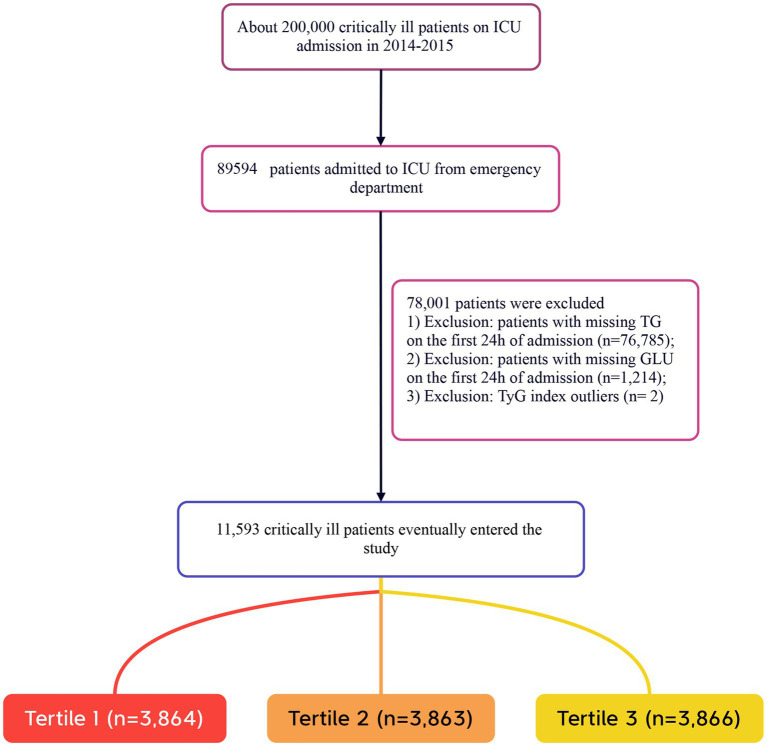
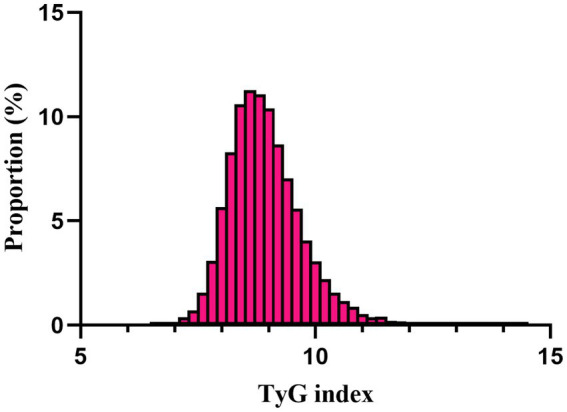
Methods: Using data from the eICU Collaborative Research Database, we conducted a retrospective multicenter cohort study of 11,593 ED-to-ICU critically ill patients. The TyG index was calculated at ED presentation. The primary outcome was 28-day all-cause mortality. Multivariable Cox regression, restricted cubic splines, and sensitivity analyses were performed to assess associations.
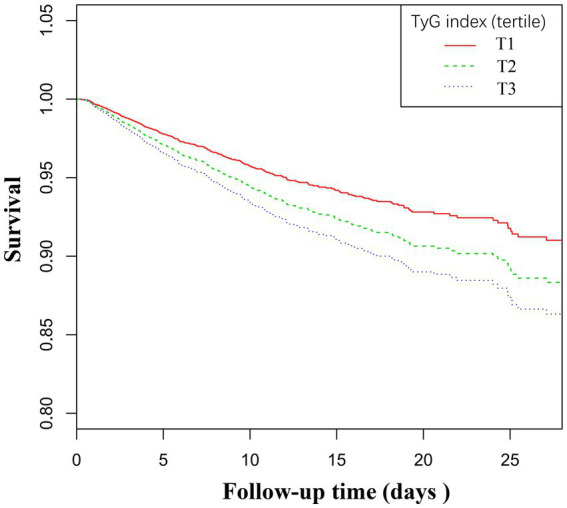
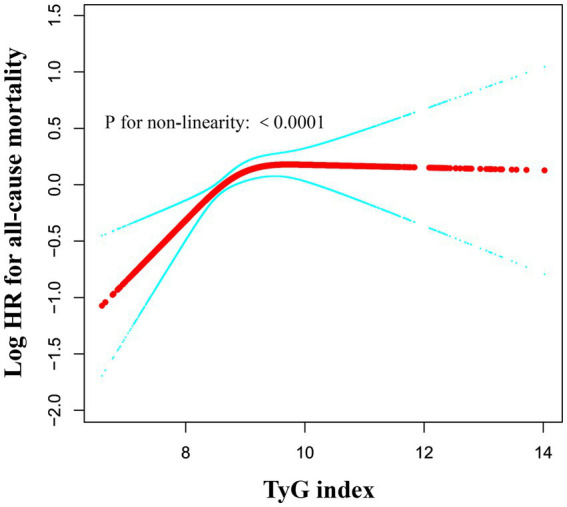
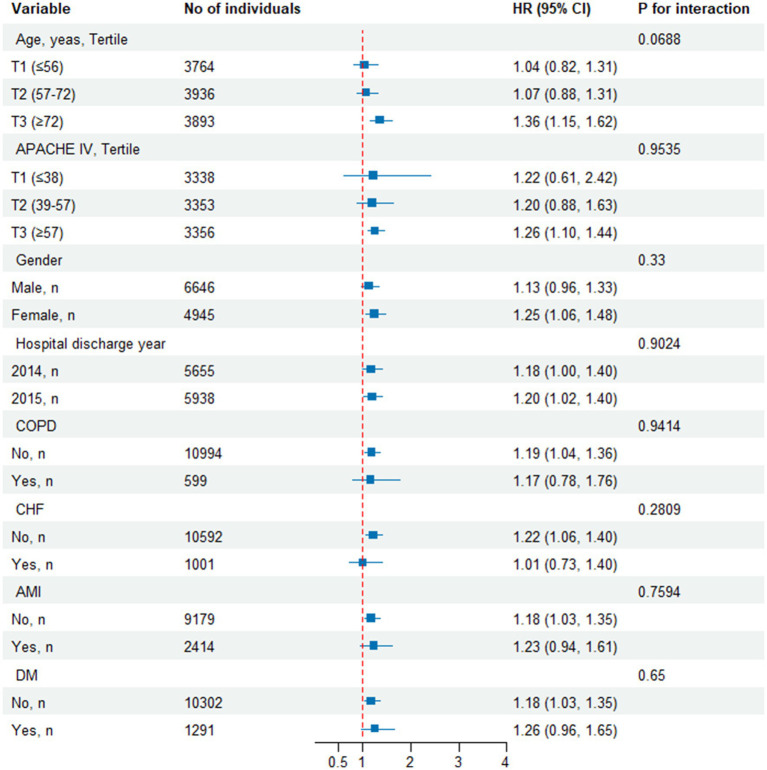
Results: Among patients (mean age 63.6 ± 15.7 years, 57.3% male), 28-day mortality was 6.96%. The relationship between the TyG index and mortality was nonlinear, featuring a critical threshold at a TyG index value of 9.84. Below this cutoff, each unit increase in TyG index significantly elevated mortality risk (HR 1.47, 95% CI 1.20-1.69, p < 0.0001), while above it, the risk plateaued (HR 1.04, 95% CI 1.03-1.05, p = 0.097). The association remained robust after adjustment for confounders (adjusted HR 1.19, 95% CI 1.04-1.35, p = 0.0089) and across sensitivity analyses.
Conclusion: The TyG index, readily obtainable at ED presentation, provides emergency clinicians with a practical tool for early mortality risk stratification in critically ill patients. Its nonlinear association with 28-day mortality suggests a saturation effect, enabling rapid identification of high-risk patients who may benefit from intensified monitoring and intervention.
Keywords: ICU admission; emergency critical care; insulin resistance; mortality prediction; risk stratification; triglyceride-glucose index.
Copyright © 2025 Huang, Bu, Yu, Gu and Yin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Association between trajectory of triglyceride-glucose index and all-cause mortality in critically ill patients with atrial fibrillation: a retrospective cohort study.Cardiovasc Diabetol. 2025 Jul 10;24(1):278. doi: 10.1186/s12933-025-02838-x. Cardiovasc Diabetol. 2025. PMID: 40640797 Free PMC article.
-
Association between triglyceride-glucose index and mortality in critically ill patients with atrial fibrillation: a retrospective cohort study.Cardiovasc Diabetol. 2025 Mar 24;24(1):138. doi: 10.1186/s12933-025-02697-6. Cardiovasc Diabetol. 2025. PMID: 40128768 Free PMC article.
-
Association between triglyceride-glucose-body mass index and adverse prognosis in elderly patients with severe heart failure and type 2 diabetes: a retrospective study based on the MIMIC-IV database.Cardiovasc Diabetol. 2025 Jul 24;24(1):299. doi: 10.1186/s12933-025-02870-x. Cardiovasc Diabetol. 2025. PMID: 40707996 Free PMC article.
-
Does diabetes status modify the association between the triglyceride-glucose index and major adverse cardiovascular events in patients with coronary heart disease? A systematic review and meta-analysis of longitudinal cohort studies.Cardiovasc Diabetol. 2025 Aug 4;24(1):317. doi: 10.1186/s12933-025-02890-7. Cardiovasc Diabetol. 2025. PMID: 40760488 Free PMC article.
-
Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients.Cochrane Database Syst Rev. 2015 Jan 8;1(1):CD010225. doi: 10.1002/14651858.CD010225.pub2. Cochrane Database Syst Rev. 2015. PMID: 25568981 Free PMC article.
References
-
- McDowald K, Direktor S, Hynes EA, Sahadeo A, Rogers ME. Effectiveness of collaboration between emergency department and intensive care unit teams on mortality rates of patients presenting with critical illness: a systematic review. JBI Database System Rev Implement Rep. (2017) 15:2365–89. doi: 10.11124/JBISRIR-2017-003365, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources