

Microangiopathic Anemia
- PMID: 40809448
- PMCID: PMC12342704
- DOI: 10.1159/000544724
Microangiopathic Anemia
Abstract
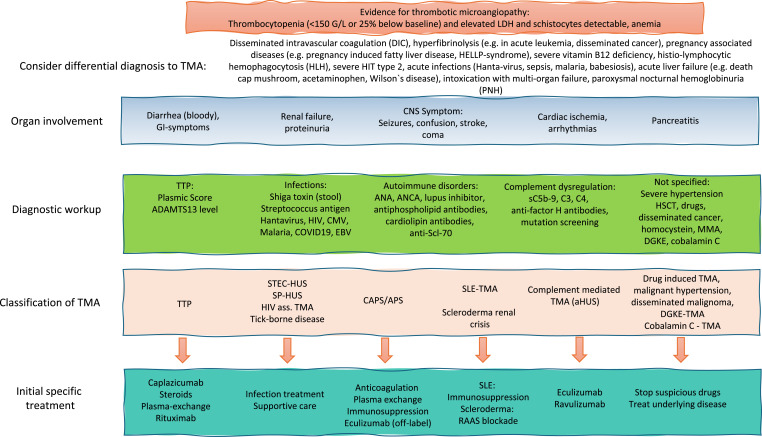
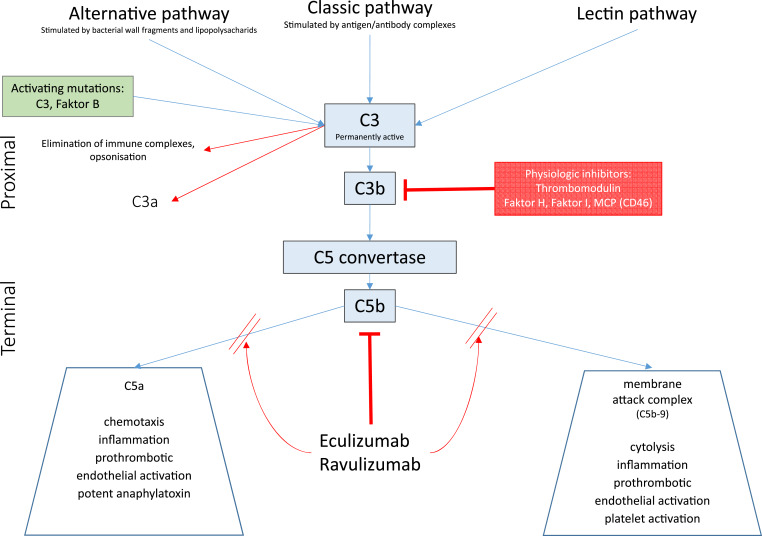
Background: Patients suffering from hemolytic anemia, thrombocytopenia, and organ damage may suffer from microangiopathic anemia, also called thrombotic microangiopathy (TMA). This condition is caused by many different pathogenic mechanisms and is always life-threatening due to vessel occlusion in vital organs. Rapid and careful workup is mandatory to identify the cause of TMA. To identify patients suffering from immune-mediated thrombotic thrombocytopenic purpura (iTTP), ADAMTS13 (a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13) measurement is mandatory. All patients with ADAMTS13 activity below 10 IU/dL are assigned to the diagnosis iTTP and need urgent targeted treatment. Meanwhile, caplacizumab - an anti-von Willebrand factor humanized single-variable-domain immunoglobulin fragment - is approved for the treatment of iTTP. Patients with TMA and ADAMTS13 activity>10 IU/dL can be assigned to other forms of TMA such as hemolytic uremic syndrome (HUS), complement-mediated TMA (cmTMA) - previously assigned to the term atypical HUS (aHUS) - or TMA secondary to underlying diseases such as autoimmune disorders, cancer, or infectious diseases. Complement inhibition with C5 targeted treatment, such as eculizumab or ravulizumab, is approved for the treatment of cmTMA. Even more challenging may be the differential diagnosis in pregnancy, in cancer patients with complex medication and the need to rule out conditions imitating TMA such as Evans syndrome, intoxication, infection, or severe vitamin B12 deficiency.
Summary: Identifying TMA and defining the pathophysiology of TMA is urgently necessary in patients with thrombocytopenia and hemolytic anemia with or without obvious organ damage.
Key message: ADAMTS13 testing is the most important specific test to classify TMA.
Keywords: Hemolytic uremic syndrome; Thrombotic microangiopathy; Thrombotic thrombocytopenic purpura.
© 2025 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
M.B. has received honoraria from Alexion, Sanofi, and Takeda. J.B. states no conflict of interest.
Figures
Similar articles
-
Genetic Atypical Hemolytic-Uremic Syndrome.2007 Nov 16 [updated 2021 Sep 23]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. 2007 Nov 16 [updated 2021 Sep 23]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. PMID: 20301541 Free Books & Documents. Review.
-
Immune Thrombotic Thrombocytopenic Purpura: A Review.JAMA. 2025 Aug 12;334(6):517-529. doi: 10.1001/jama.2025.3807. JAMA. 2025. PMID: 40388146 Review.
-
Microangiopathic Hemolytic Anemia and Thrombocytopenia in Patients With Cancer.J Oncol Pract. 2016 Jun;12(6):523-30. doi: 10.1200/JOP.2016.012096. J Oncol Pract. 2016. PMID: 27288467
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
A case-based narrative review of pregnancy-associated atypical hemolytic uremic syndrome/complement-mediated thrombotic microangiopathy.Kidney Int. 2024 May;105(5):960-970. doi: 10.1016/j.kint.2023.12.021. Epub 2024 Feb 24. Kidney Int. 2024. PMID: 38408703 Free PMC article.
References
-
- Shatzel JJ, Taylor JA. Syndromes of thrombotic microangiopathy. Med Clin North Am. 2017;101(2):395–415. - PubMed
-
- Amorosi EL, Ultmann JE. Thrombotic thrombozytopenic purpura: report of 16 cases and review of the literature. Medicine. 1966;45(2):139–60.
-
- Rock GA, Shumak KH, Buskard NA, Blanchette VS, Kelton JG, Nair RC, et al. Comparison of plasma exchange with plasma infusion in the treatment of thrombotic thrombocytopenic purpura. Canadian Apheresis Study Group. N Engl J Med. 1991;325(6):393–7. - PubMed
-
- Leisring J, Brodsky SV, Parikh SV. Clinical evaluation and management of thrombotic microangiopathy. Arthritis Rheumatol. 2024;76(2):153–65. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
