

The Evolving Field of Regenerative Aesthetics: A Review and Case Series
- PMID: 40809631
- PMCID: PMC12344607
- DOI: 10.7759/cureus.87878
The Evolving Field of Regenerative Aesthetics: A Review and Case Series
Abstract
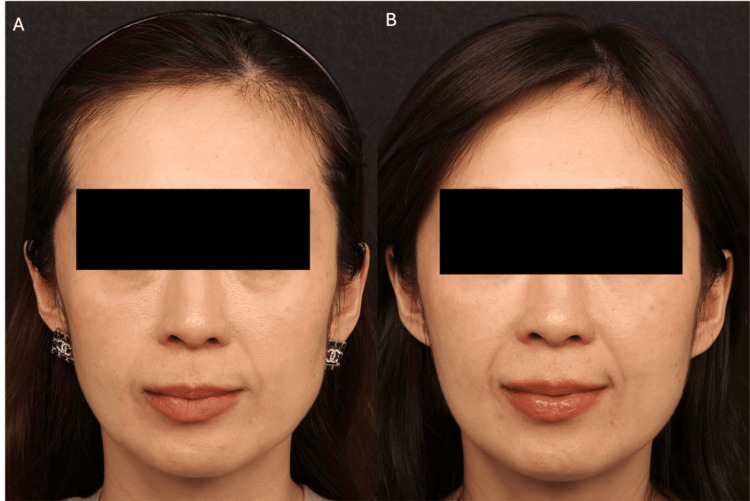
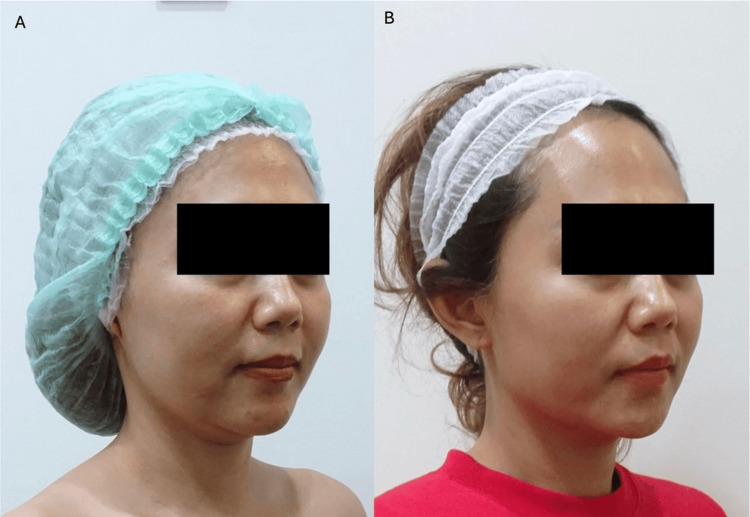
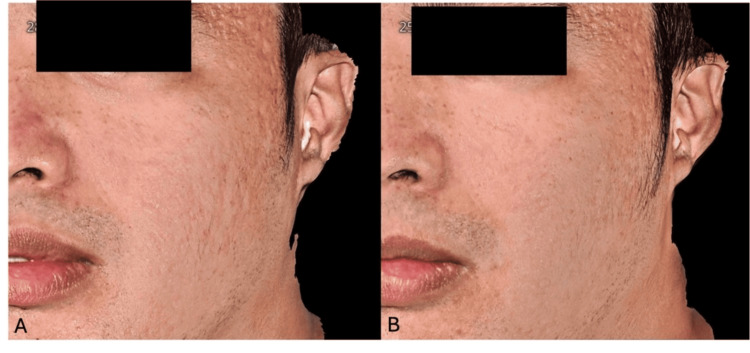
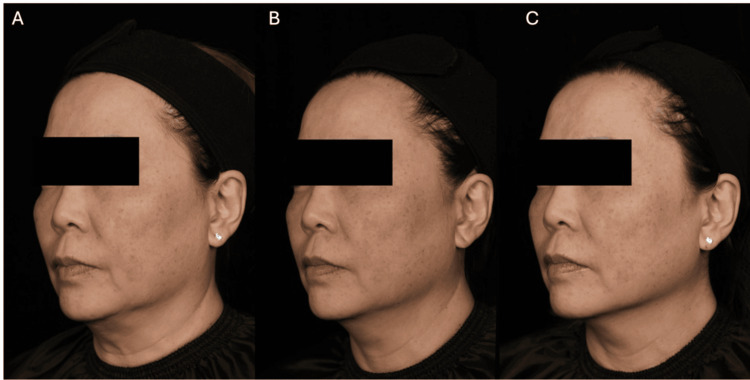
Dermal fillers such as calcium hydroxyapatite-carboxymethylcellulose (CaHA-CMC), polycaprolactone (PCL), and poly-l-lactic acid (PLLA) are increasingly used as 'biostimulators' to stimulate native collagen production for longer-lasting aesthetic improvement. Volume replacement should, ideally, renew local tissue architectures and functions, but the replaced volume may not align structurally or functionally with the original tissue. The ability to achieve this regenerative, biostimulatory aesthetic rejuvenation requires a thorough understanding of the principles and mechanisms of tissue regeneration and its proper application. We reviewed the concepts of regenerative medicine, regenerative aesthetics, and biostimulation in the context of PLLA and CaHA and discussed the effects on immunological pathways and neocollagenesis when these materials are used as biostimulators in clinical aesthetics. Additionally, to understand how the concept of regenerative aesthetics is applied in the real world, we present cases demonstrating best practices and outcomes when using CaHA-CMC in a group of 11 Asian patients. Asian physicians' practices with CaHA-CMC have evolved beyond its volumizing and contouring benefits to its ability to induce regeneration in aging tissues. This has been achieved through the use of CaHA-CMC as monotherapy or in combination with other modalities. Moreover, CaHA-CMC allows physicians to offer a single, minimally invasive product to patients seeking treatment for skin laxity, wrinkles, crepiness, and volume loss while achieving multiple visible aesthetic improvements. Unlike conventional dermal fillers, the ability to leverage the regenerative qualities of CaHA-CMC effectively resolves age-related aesthetic issues in a durable manner using their body's own systems, allowing patients to emphasize their own unique features.
Keywords: asian; biostimulation; calcium hydroxyapatite; collagen; inflammation; regeneration.
Copyright © 2025, Corduff et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: Funding for manuscript editing and preparation was provided by Merz Asia Pacific Pte Ltd to Dr Shawna Tan, Medical Writers Asia. Niamh Corduff is a clinical advisor and lecturer for Merz Aesthetics. All other authors report no conflicts of interest related to this manuscript. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures


Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
A Systematic Review on the Effectiveness and Safety of Combining Biostimulators with Botulinum Toxin, Dermal Fillers, and Energy-Based Devices.Aesthetic Plast Surg. 2025 May;49(10):2809-2833. doi: 10.1007/s00266-024-04627-5. Epub 2024 Dec 24. Aesthetic Plast Surg. 2025. PMID: 39719485
-
Microfocused Ultrasound With Visualization (MFU-V) and Hyperdilute Calcium Hydroxylapatite (CaHA-CMC) of the Lower Face and Submentum to Treat Skin Laxity: A Pilot Study Demonstrating Superiority of MFU-V First Followed by Hyperdilute CaHA-CMC.Aesthet Surg J. 2025 Feb 18;45(3):305-312. doi: 10.1093/asj/sjae226. Aesthet Surg J. 2025. PMID: 39511699 Clinical Trial.
-
Minimally Invasive Facial Rejuvenation with the Hybrid Filler HArmonyCa™.Aesthetic Plast Surg. 2024 Dec;48(23):5251-5253. doi: 10.1007/s00266-023-03649-9. Epub 2023 Oct 9. Aesthetic Plast Surg. 2024. PMID: 37814039
-
Management of urinary stones by experts in stone disease (ESD 2025).Arch Ital Urol Androl. 2025 Jun 30;97(2):14085. doi: 10.4081/aiua.2025.14085. Epub 2025 Jun 30. Arch Ital Urol Androl. 2025. PMID: 40583613 Review.