

Long-term outcomes of dupilumab therapy in severe asthma: A retrospective, multicenter, real-world study
- PMID: 40810090
- PMCID: PMC12347924
- DOI: 10.1016/j.jacig.2025.100533
Long-term outcomes of dupilumab therapy in severe asthma: A retrospective, multicenter, real-world study
Abstract
Background: Dupilumab is an IL-4Rα antibody approved for treatment of severe asthma. Real-world data on the continuation and cessation patterns of dupilumab and long-term treatment efficacy are scarce.
Objective: We sought to analyze real-world, long-term treatment outcomes and to evaluate trajectories of patients continuing or discontinuing dupilumab therapy over a 3-year period.
Methods: This multicenter, retrospective, real-world cohort study included patients with severe asthma who started dupilumab before March 2021. Data on asthma control, medication, lung function, and annualized exacerbation rates were collected at baseline and 3, 12, and 36 months after initiation of dupilumab therapy. Asthma remission was assessed at 12 months and 36 months after dupilumab initiation.
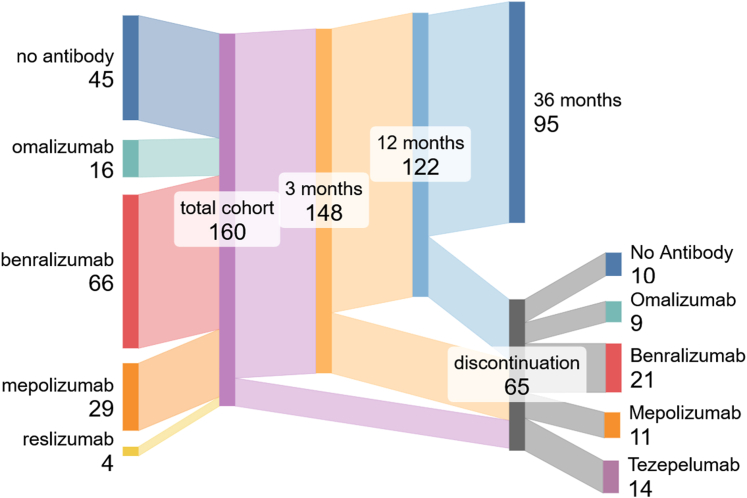
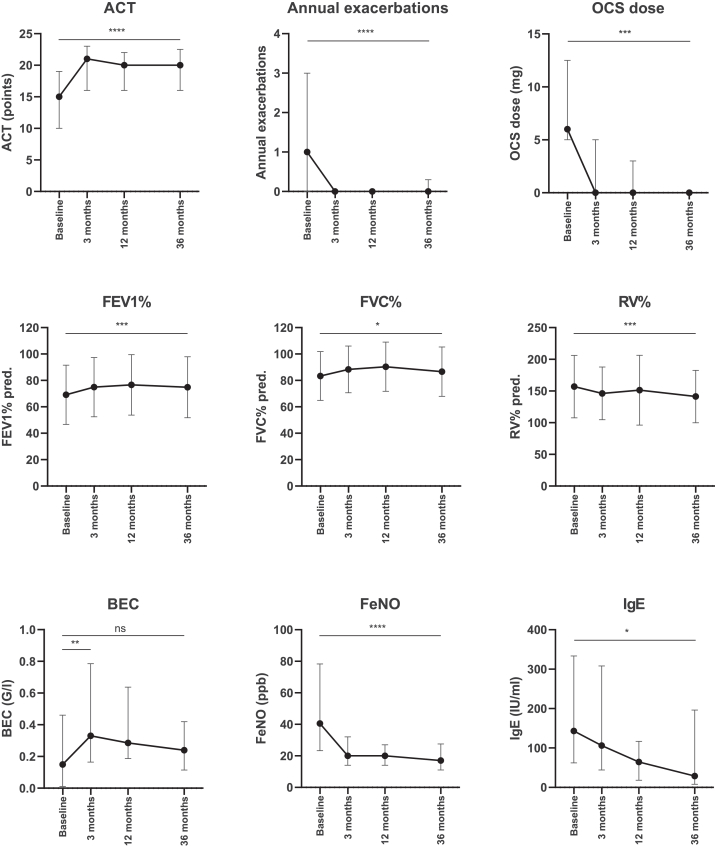
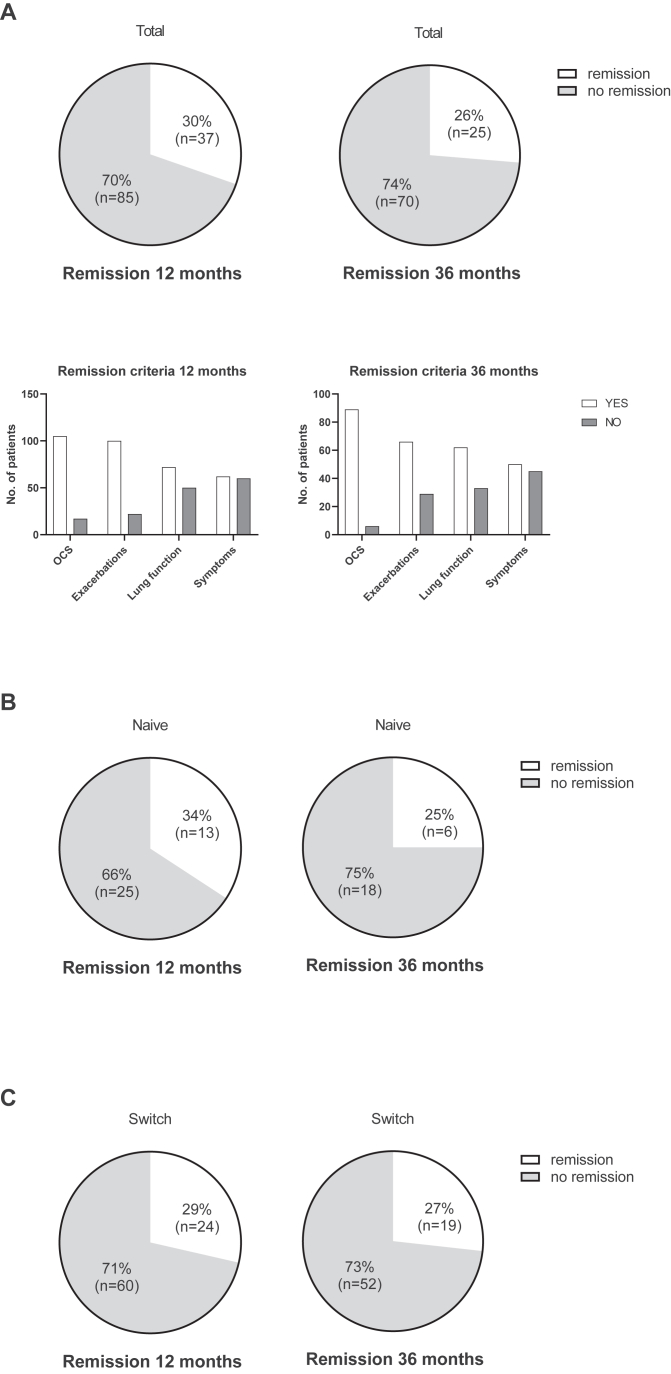
Results: Of 160 included patients, 95 patients (59%) continued dupilumab therapy for 36 months; 65 patients (41%) discontinued therapy after a median time of therapy of 8 months. Patients who continued dupilumab for 36 months had significant reductions in annual exacerbations (-1; P < .0001) and oral corticosteroid dose (-5.5 mg/day; P < .001) as well as significant improvements in asthma control (asthma control test +5; P < .0001) and lung function (percent predicted of FEV1 +7%; P < .001) compared with baseline. Of patients who continued dupilumab, 30% achieved remission at 12 months, and 26% achieved remission at 36 months. Of the 65 patients who discontinued therapy, 55 switched to another antibody, and 10 did not receive further antibody treatment.
Conclusions: Dupilumab represents an effective long-term treatment option for patients with severe asthma, with sustained treatment effects up to 36 months. Importantly, a relevant proportion of patients achieved remission in this pretreated population.
Keywords: Severe asthma; antibody; dupilumab; long-term; real-world.
© 2025 The Author(s).
Conflict of interest statement
The authors received no funding for the submitted work Disclosure of potential conflict of interest: C. Mümmler reports personal fees and speaker fees from Sanofi and AstraZeneca, outside the submitted work. A. Lenoir reports personal fees from 10.13039/501100015086AOP Health, 10.13039/100004339Sanofi, and 10.13039/100004325AstraZeneca, outside the submitted work. J. Götschke reports personal fees and speaker fees from 10.13039/100004331Johnson & Johnson and AstraZeneca. M. Gerckens received a travel grant from Chiesi outside the submitted work. M. Kayser reports honoraria for lectures from AstraZeneca and GSK, outside the submitted work. N. Drick reports honoraria for lectures and consultation from AstraZeneca, GSK, and Sanofi, outside the submitted work. H. Suhling reports personal fees/speaker honoraria from AstraZeneca, GSK, Novartis, and Sanofi, all outside the submitted work. L. Biener reports personal fees and speaker fees from AstraZeneca, Boehringer Ingelheim, and Sanofi, all outside the submitted work. D. Skowasch reports fees for lectures or consultations from AstraZeneca, Boehringer Ingelheim, GSK, Janssen, MSD, Sanofi, all outside the submitted work. N. Kneidinger reports personal fees and speaker fees from GSK and AstraZeneca, outside the submitted work. J. Behr reports honoraria for lectures and consultation from AstraZeneca, Boehringer-Ingelheim, BMS, Gossamer Bio, Sanofi, United Therapeutics, Ferrer, and Novartis, outside the submitted work. K. Milger received speaker and/or advisor fees from AstraZeneca, Chiesi, Insmed, GSK, Novartis, Sanofi. The rest of the authors declare that they have no relevant conflicts of interest.
Figures
References
-
- Porsbjerg C., Melén E., Lehtimäki L., Shaw D. Asthma. Lancet. 2023;401:858–873. - PubMed
-
- Chung K.F., Wenzel S.E., Brozek J.L., Bush A., Castro M., Sterk P.J., et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43:343–373. - PubMed
-
- 2024 Main Report. Global Initiative for Asthma. 2024. https://ginasthma.org/2024-report/ Available at:
-
- Robinson D., Humbert M., Buhl R., Cruz A.A., Inoue H., Korom S., et al. Revisiting type 2-high and type 2-low airway inflammation in asthma: current knowledge and therapeutic implications. Clin Exp Allergy. 2017;47:161–175. - PubMed
-
- Mümmler C., Milger K. Biologics for severe asthma and beyond. Pharmacol Ther. 2023;252 - PubMed
LinkOut - more resources
Full Text Sources
