

Constructing the first comorbidity networks in companion dogs in the Dog Aging Project
- PMID: 40811246
- PMCID: PMC12352663
- DOI: 10.1371/journal.pcbi.1012728
Constructing the first comorbidity networks in companion dogs in the Dog Aging Project
Abstract
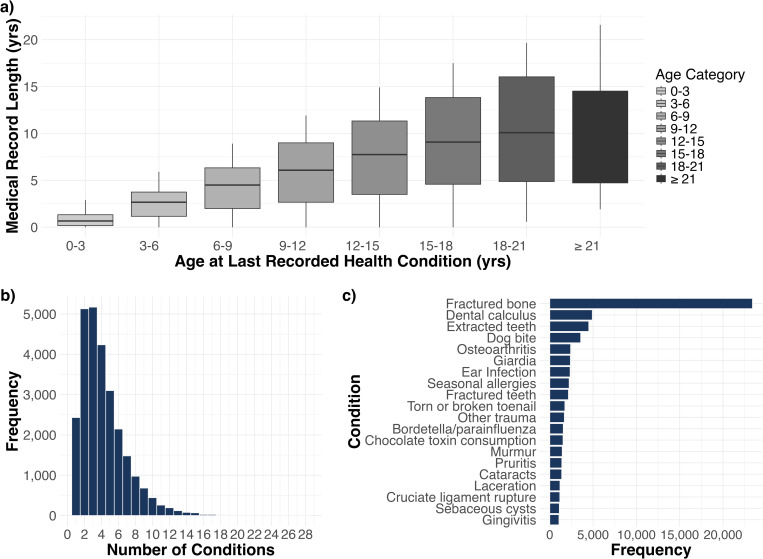
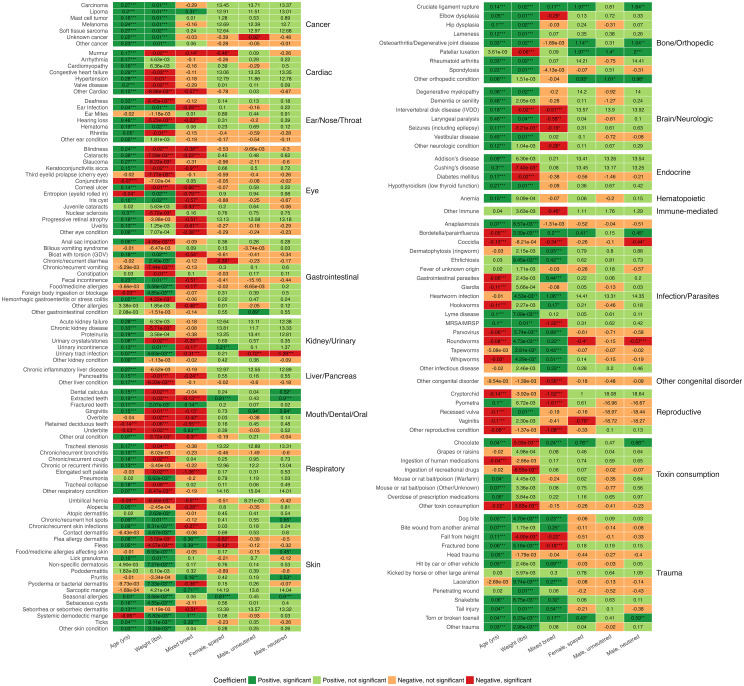
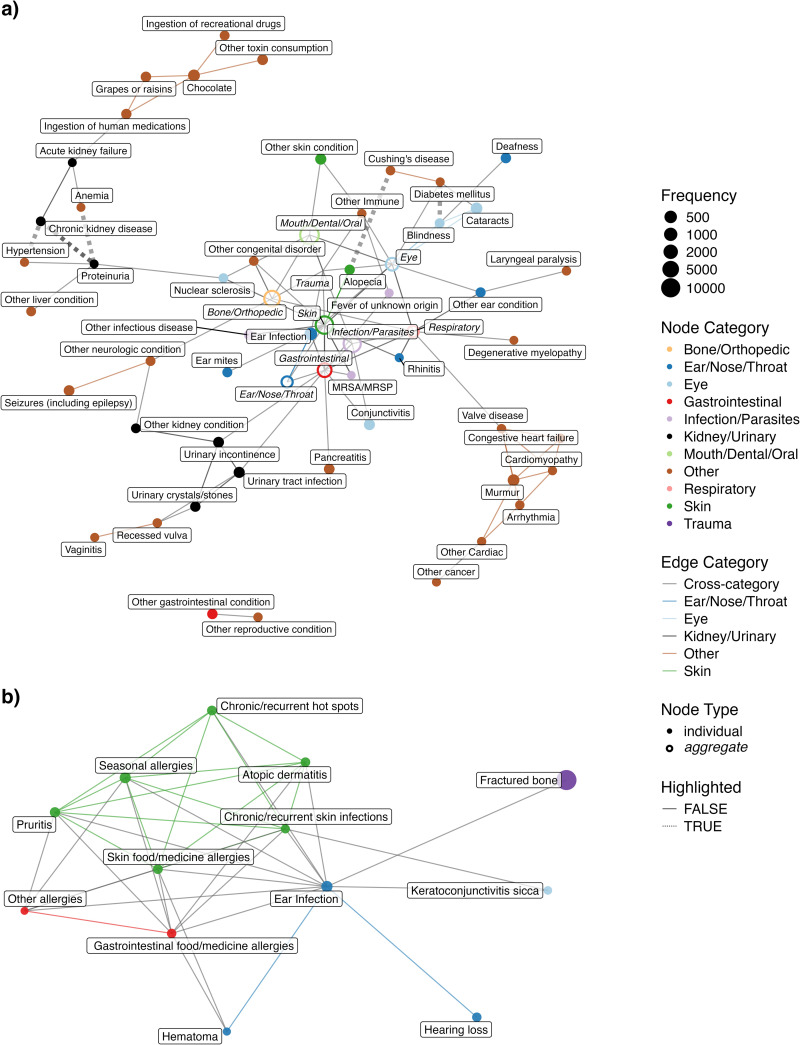
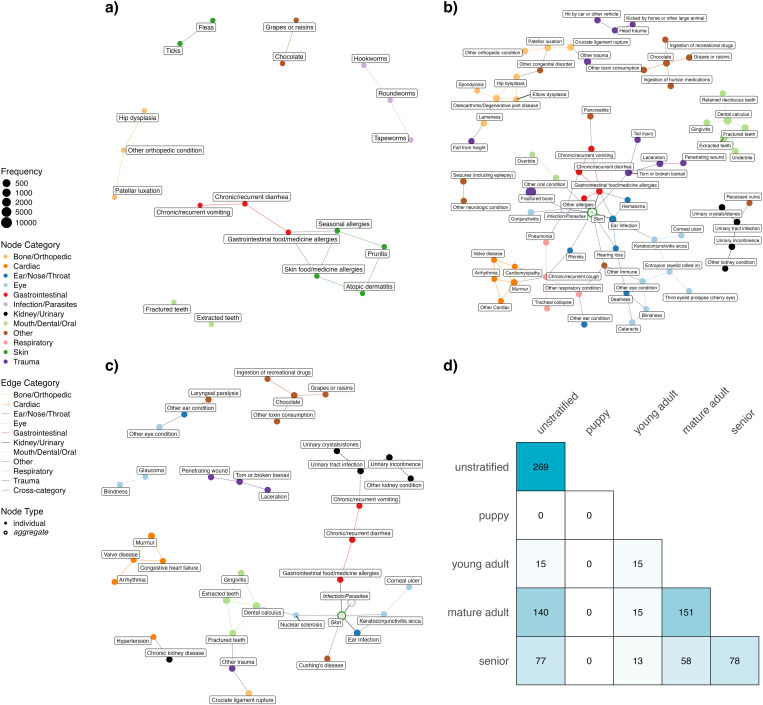
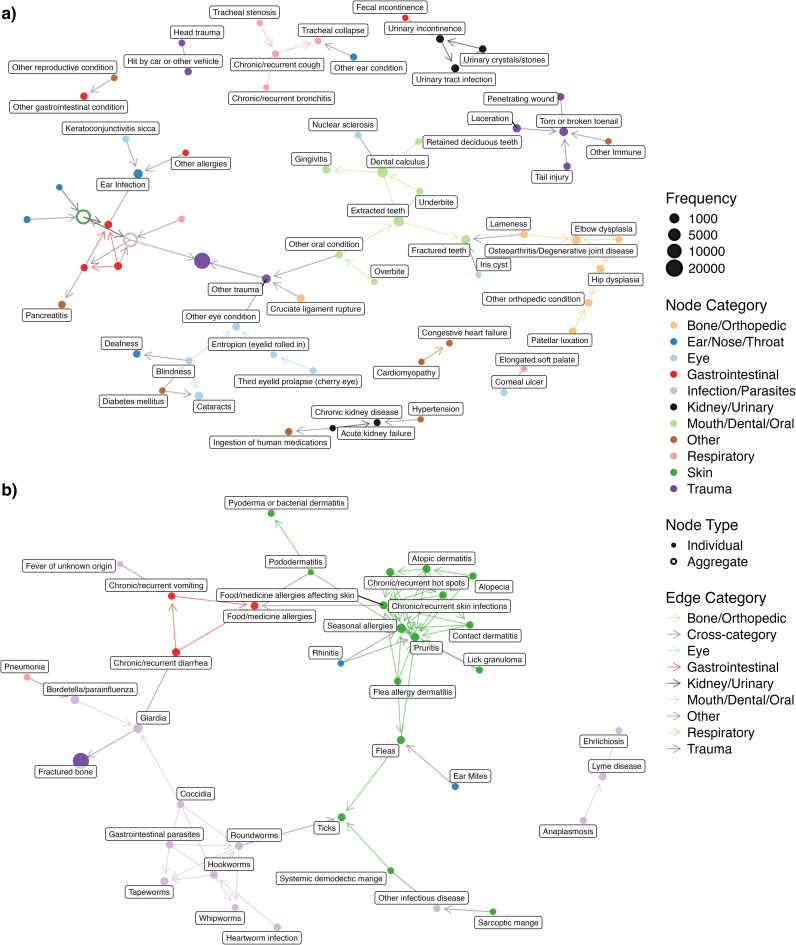
Comorbidity and its association with age are of great interest in geroscience. However, there are few model organisms that are well-suited to study comorbidities that will have high relevance to humans. In this light, we turn our attention to the companion dog. The companion dog shares many morbidities with humans. Thus, a better understanding of canine comorbidity relationships could benefit both humans and dogs. We present an analysis of canine comorbidity networks from the Dog Aging Project, a large epidemiological cohort study of companion dogs in the United States. We included owner-reported health conditions that occurred in at least 60 dogs (n = 160) and included only dogs that had at least one of those health conditions (n = 26,614). We constructed an undirected comorbidity network using a Poisson binomial test, adjusting for age, sex, sterilization status, breed background (i.e., purebred vs. mixed-breed), and weight. The comorbidity network reveals well-documented comorbidities, such as diabetes with cataracts and blindness, and hypertension with chronic kidney disease (CKD). In addition, this network also supports less well-studied comorbidity relationships, such as proteinuria with anemia. A directed comorbidity network accounting for time of reported condition onset suggests that diabetes precedes cataracts, elbow/hip dysplasia before osteoarthritis, and keratoconjunctivitis sicca before corneal ulcer, which are consistent with the canine literature. Analysis of age-stratified networks reveals that global centrality measures increase with age and are the highest in the Senior group compared to the Young Adult and Mature Adult groups. Only the Senior group identified the association between hypertension and CKD. Our results suggest that comorbidity network analysis is a promising method to enhance clinical knowledge and canine healthcare management.
Copyright: © 2025 Fang et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: DP is a paid consultant of WndrHLTH Club, Inc. and Infinity Research Labs.
Figures
Update of
-
Constructing the first comorbidity networks in companion dogs in the Dog Aging Project.bioRxiv [Preprint]. 2025 Jul 11:2024.12.18.629088. doi: 10.1101/2024.12.18.629088. bioRxiv. 2025. Update in: PLoS Comput Biol. 2025 Aug 14;21(8):e1012728. doi: 10.1371/journal.pcbi.1012728. PMID: 39763936 Free PMC article. Updated. Preprint.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
