

Impact of Charlson Comorbidity Index on clinical outcomes of patients with non-ST segment elevation acute coronary syndrome: a propensity score matching method
- PMID: 40812824
- PMCID: PMC12352207
- DOI: 10.1136/bmjopen-2024-097359
Impact of Charlson Comorbidity Index on clinical outcomes of patients with non-ST segment elevation acute coronary syndrome: a propensity score matching method
Abstract
Objective: Patients with non-ST segment elevation acute coronary syndrome (NSTEACS) admitted into emergency department are usually combined with a high number of comorbidities. Charlson Comorbidity Index (CCI) is the most commonly used measure to assess comorbidity in clinical practice. However, the impact of CCI on the clinical outcomes of patients with NSTEACS are still unclear.
Design: A multicenter retrospective cohort study.
Setting: We used data from the Chongqing Medical University Medical Data Science Academy in Chongqing, China, which contains data from seven tertiary hospitals.
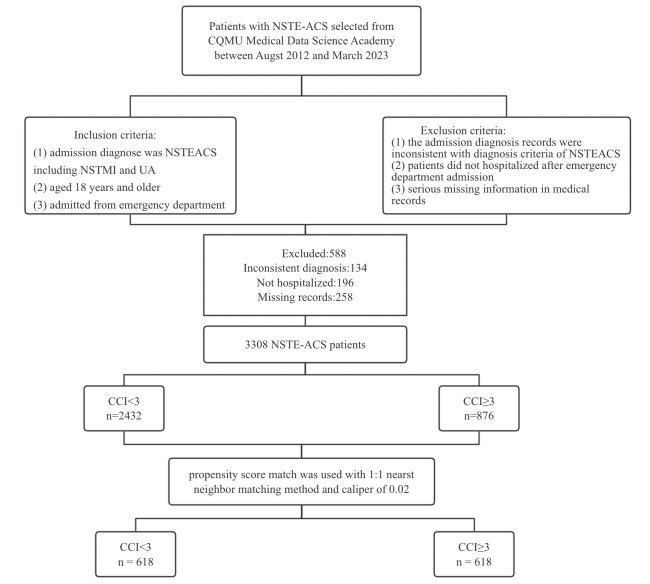
Participants: Data from 3308 consecutive patients aged over 18 diagnosed with NSTEACS admitted to emergency departments of seven hospitals from August 2012 to March 2023 were retrospectively analysed.
Methods: Patients were divided into two groups based on CCI: CCI <3 as low CCI, and CCI ≥3 as high CCI. A propensity score matching (PSM) analysis using the 1:1 nearest neighbour matching method with a calliper value of 0.02 was adopted to control for differences between the comparison cohorts. Univariate and multivariate logistic regression analyses were carried out to produce ORs with 95% CIs to identify whether the CCI is a potential independent predictor of in-hospital outcomes in the matched cohort.
Primary and secondary outcome measures: In-hospital mortality rate, major adverse cardiovascular events (MACEs), length of stay and readmission rate.
Results: 876 and 2432 patients belonged to the high CCI group (CCI ≥3) and the low CCI group (CCI <3). After PSM, 618 pairs were matched. There were significant differences in sociodemographic, clinical characteristics and laboratory tests between the two groups before PSM. The results were balanced and comparable after PSM (p>0.05). In patients with high CCI, in-hospital mortality, the incidence of MACEs, length of stay (LOS) and readmission rate were significantly higher compared with those with low CCI. Univariate analysis revealed that a higher CCI was associated with an increased incidence of MACEs, prolonged LOS and a higher readmission rate. Multivariate analysis demonstrated that even after adjusting for various confounding factors, a higher CCI remained an independent risk factor for an increased incidence of MACEs, prolonged LOS and higher readmission rate.
Conclusion: A high CCI not only increases the risk of in-hospital MACEs but also prolongs the length of stay and increases the readmission rate. We recommend that the CCI be used as a crucial risk indicator for clinical practitioners to identify and manage patients with a poor prognosis.
Keywords: Coronary heart disease; Multimorbidity; Prognosis.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures

Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
High Risk of Readmission After THA Regardless of Functional Status in Patients Discharged to Skilled Nursing Facility.Clin Orthop Relat Res. 2024 Jul 1;482(7):1185-1192. doi: 10.1097/CORR.0000000000002950. Epub 2024 Jan 16. Clin Orthop Relat Res. 2024. PMID: 38227380 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
References
-
- Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130:2354–94. doi: 10.1161/CIR.0000000000000133. - DOI - PubMed
-
- Beska B, Mills GB, Ratcovich H, et al. Impact of multimorbidity on long-term outcomes in older adults with non-ST elevation acute coronary syndrome in the North East of England: a multi-centre cohort study of patients undergoing invasive care. BMJ Open. 2022;12:e061830. doi: 10.1136/bmjopen-2022-061830. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous