

Treatment disparities and prognostic implications in octogenarians versus non-octogenarians with high-gradient severe aortic stenosis
- PMID: 40813105
- PMCID: PMC12352216
- DOI: 10.1136/openhrt-2025-003405
Treatment disparities and prognostic implications in octogenarians versus non-octogenarians with high-gradient severe aortic stenosis
Abstract
Background: Aortic valve replacement (AVR) is considered one of the most potent disease-modifying procedures among patients with severe aortic stenosis (sAS). Accordingly, we have witnessed a consistent increase in the procedure rates in recent years. Nevertheless, the elderly population, particularly octogenarians, remains relatively undertreated. The current study aims to document the disparities in AVR rates among octogenarians and its prognostic significance.
Methods: A vast database of Maccabi Health Services, the second largest health maintenance organisation in Israel, counting nearly 2.8 million members, was retrospectively analysed from 2005 to 2021 for all patients over 60 years, with a detailed echocardiography report compatible with a diagnosis of high-gradient sAS. The database was extracted using the MDClone healthcare data platform, generating synthetic data reliably representing the original population. All-cause mortality was set to be the primary outcome, and survival models using adjusted multivariable analyses for several clinical and echocardiographic parameters were applied.
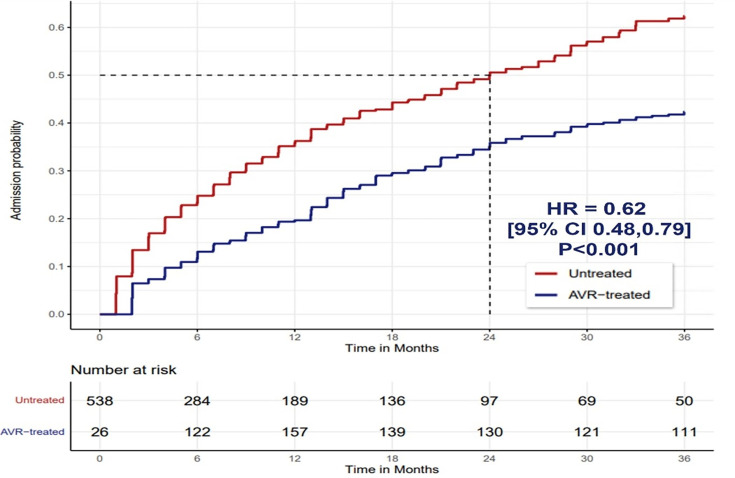
Results: The cohort consisted of 1396 patients with high-gradient sAS (76±7 years) with 39% octogenarians. Octogenarians were less likely to undergo AVR (42% vs 60%, p<0.01) and presented more severe clinical profiles. AVR significantly reduced mortality and hospitalisations in both age groups, but octogenarians showed a pronounced survival benefit regardless of symptom status. A time-dependent analysis showed that AVR was associated with reduced all-cause mortality (HR 0.30, 95% CI 0.23 to 0.41, p<0.001) within the octogenarian group in 5 years. A similar protective effect was shown in the non-octogenarian group (HR 0.32, 95% CI 0.22 to 0.46, p<0.001).
Conclusion: This study highlights significant treatment disparities in AVR among octogenarians with high-gradient sAS despite clear benefits in survival and reduced hospitalisations. The findings suggest the need for more inclusive treatment strategies, particularly for older patients, and underscore the importance of AVR in improving clinical outcomes in this population.
Keywords: Aortic Valve Stenosis; Epidemiology; Heart Valve Diseases.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: OS, OR and CP are employees of Edwards Lifesciences.
Figures


Similar articles
-
Early Stroke Volume Variation After Transcatheter or Surgical Aortic Valve Replacement Predicts Clinical Outcomes in Low-Flow Aortic Stenosis.Catheter Cardiovasc Interv. 2025 Aug;106(2):1012-1022. doi: 10.1002/ccd.31654. Epub 2025 Jun 2. Catheter Cardiovasc Interv. 2025. PMID: 40457610 Free PMC article.
-
Sex-Associated Disparities in Surgical and Percutaneous Management of Aortic Stenosis With Severe Features: Retrospective Analysis From the National Readmission Database.J Am Heart Assoc. 2025 May 20;14(10):e038463. doi: 10.1161/JAHA.124.038463. Epub 2025 May 15. J Am Heart Assoc. 2025. PMID: 40371608 Free PMC article.
-
Long-term clinical outcomes in adult congenital aortic stenosis: results from a national study.Open Heart. 2025 Aug 27;12(2):e003534. doi: 10.1136/openhrt-2025-003534. Open Heart. 2025. PMID: 40866083
-
Integration of Flow-Gradient Patterns Into Clinical Decision Making for Patients With Suspected Severe Aortic Stenosis and Preserved LVEF: A Systematic Review of Evidence and Meta-Analysis.JACC Cardiovasc Imaging. 2016 Nov;9(11):1255-1263. doi: 10.1016/j.jcmg.2016.01.035. Epub 2016 Aug 17. JACC Cardiovasc Imaging. 2016. PMID: 27544900
-
Early and Late Outcomes of Transcatheter Aortic Valve Replacement in Patients With Prior Chest Radiation: A Systematic Review and Meta-Analysis.Catheter Cardiovasc Interv. 2025 Apr;105(5):1012-1023. doi: 10.1002/ccd.31417. Epub 2025 Jan 22. Catheter Cardiovasc Interv. 2025. PMID: 39840647
References
-
- Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021;77:e25–197. doi: 10.1016/j.jacc.2020.11.018. - DOI - PubMed
-
- McDonagh TA, Metra M, Adamo M, et al. Corrigendum to: 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2021;42:3599–726. doi: 10.1093/eurheartj/ehab670. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical