

Genetic evaluation of pediatric pituitary adenomas and USP8-related genotype-phenotype correlations in Cushing's disease
- PMID: 40813536
- PMCID: PMC12354490
- DOI: 10.1007/s11102-025-01557-6
Genetic evaluation of pediatric pituitary adenomas and USP8-related genotype-phenotype correlations in Cushing's disease
Abstract
Purpose: Pituitary adenomas (PAs) constitute a rare pediatric diagnosis and their pathogenetic mechanisms are not clearly understood. The aim of this study was to evaluate the prevalence of genetic defects in pediatric PAs through germline and tumor testing, and to describe genotype-phenotype correlations.
Methods: Fifty-four pediatric patients with PAs and available germline and/or tumor samples were studied. Germline and/or tumor sequencing were reviewed for variants in genes previously associated with pituitary tumorigenesis.
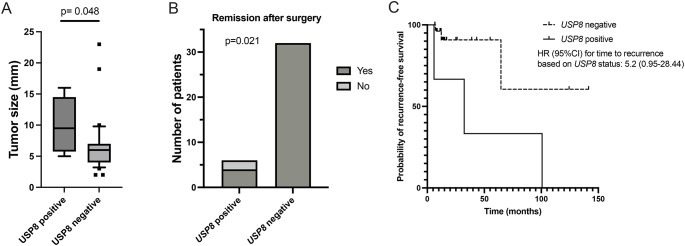
Results: Germline genetic testing revealed a pathogenic variant in AIP gene in 2 patients with growth hormone excess (GHE) and a likely pathogenic variant in CDKN2A in a patient with Cushing's disease (CD). Somatic gene sequencing identified pathogenic variants in GNAS in 4/7 patients (57.1%) with GHE. 6/38 patients (15.8%) with CD had pathogenic variants in USP8 gene, and in one tumor pathogenic variants in PRKAR1A, TP53 and MEN1 genes were identified. Overall, pathogenic/likely pathogenic germline or somatic variants were identified in 14/54 patients (25.9%). When evaluating the genotype-phenotype correlations in patients with CD, patients with somatic USP8 pathogenic variants had larger tumors (median size: 9.5 mm [6.5, 13.3] vs. 6 mm [4.0, 7.0], p = 0.048), trend towards higher incidence of cavernous sinus invasion (50% vs. 12.5%, p = 0.06), and higher risk of non-remission after surgery (33.3% vs. 0%, p = 0.021) compared to patients without USP8 variants.
Conclusions: Somatic USP8 pathogenic variants correlate with worse tumor behavior and patient outcomes in pediatric-onset CD. Unlike GH-secreting PAs, the genetic basis of the majority of pediatric corticotroph PAs remains unclear. Further studies are needed to explore the genetic drivers of pediatric CD.
Gov id: NCT00001595, NCT03206099.
Keywords: Corticotroph tumor; Cushing; Gigantism; Pediatric pituitary adenomas; Somatotroph tumor.
© 2025. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Disclosure Statement: CT received research funding for studies on treatment of abnormal growth hormone secretion by Pfizer, Inc, and for studies on treatment of Cushing’s disease by Recordati.
Figures


References
-
- Agustsson TT, Baldvinsdottir T, Jonasson JG, Olafsdottir E, Steinthorsdottir V, Sigurdsson G et al (2015) The epidemiology of pituitary adenomas in iceland, 1955–2012: a nationwide population-based study. Eur J Endocrinol 173:655–664. 10.1530/EJE-15-0189 - PubMed
-
- Broder MS, Neary MP, Chang E, Cherepanov D, Ludlam WH (2015) Incidence of Cushing’s syndrome and Cushing’s disease in commercially-insured patients < 65 years old in the United States. Pituitary 18, 283–289. 10.1007/s11102-014-0569-6 - PubMed
-
- Souteiro P, Maia R, Santos-Silva R, Figueiredo R, Costa C, Belo S et al (2019) Pituitary incidentalomas in paediatric age are different from those described in adulthood. Pituitary 22:124–128. 10.1007/s11102-019-00940-4 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
