

Visualisation and quantification of the effects of surgical humidification on intestinal perfusion and viability in a porcine model
- PMID: 40813602
- PMCID: PMC12354771
- DOI: 10.1038/s41598-025-14082-0
Visualisation and quantification of the effects of surgical humidification on intestinal perfusion and viability in a porcine model
Abstract
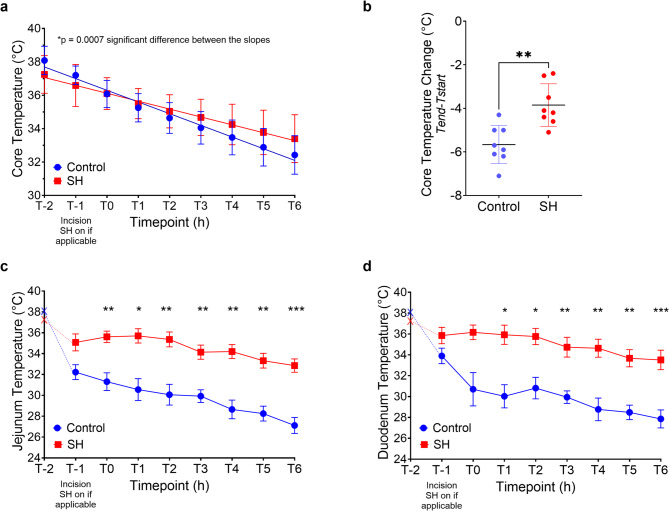
Cold and poorly oxygenated tissues are known to increase the risk of surgical site infection and anastomotic leaks in gastrointestinal surgery. Especially during laparotomy, the abdominal cavity is exposed to the cold dry operating theatre which may contribute to surgical site evaporative cooling, tissue desiccation, and reduced oxygenation. Surgical humidification, the intraoperative insufflation of warm humidified carbon dioxide into the laparotomy wound, is a local intervention designed to prevent the evaporative cooling and desiccation effects of laparotomy. In this study, we present the first data from a large animal model to visualise and quantify the effects of surgical humidification on intestinal tissue viability and oxygenation during open surgery. Our results demonstrated that surgical humidification significantly improved core and local intestinal temperature. In addition, intestinal local capillary lactate levels used as a surrogate of local tissue oxygenation demonstrated a significant improvement with surgical humidification. Further, surgical humidification showed a significant protective effect against peritoneal and intestinal tissue damage. The use of surgical humidification improved local tissue oxygenation as confirmed with perfusion biomarkers, as well as maintaining core and local temperature repetition. Surgical humidification may help to improve outcomes of abdominal open surgery. Further confirmatory clinical trials are needed.
Keywords: Humidification; Laparotomy; Surgery; Surgical site infection.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: EN has given paid lectures for Fisher & Paykel. All other authors have no conflicts of interest or financial ties to disclose.
Figures




References
-
- Delin, N. A. et al. J. Thorac. Cardiovasc. Surg.49, 511–516 https://doi.org:10.1016/S0022-5223(19)33287-8 (1965).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
