

HIBRID: histology-based risk-stratification with deep learning and ctDNA in colorectal cancer
- PMID: 40813777
- PMCID: PMC12354865
- DOI: 10.1038/s41467-025-62910-8
HIBRID: histology-based risk-stratification with deep learning and ctDNA in colorectal cancer
Abstract
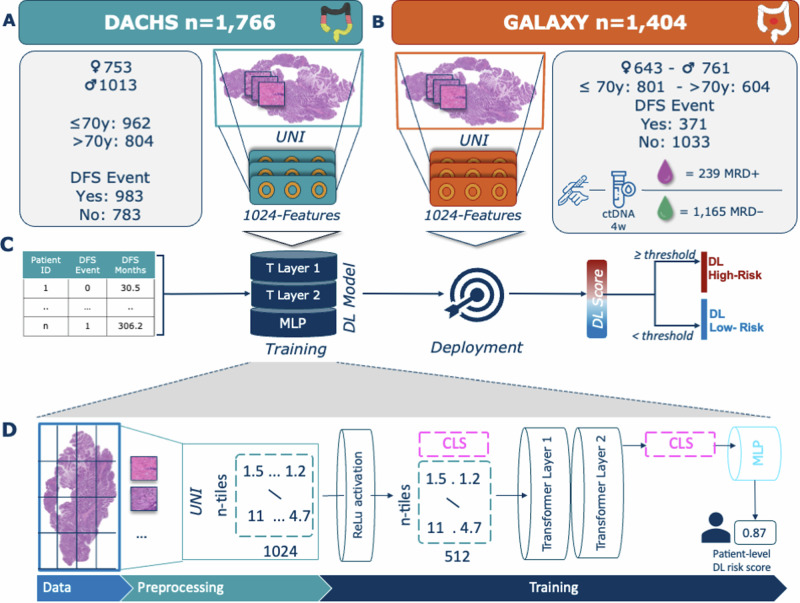
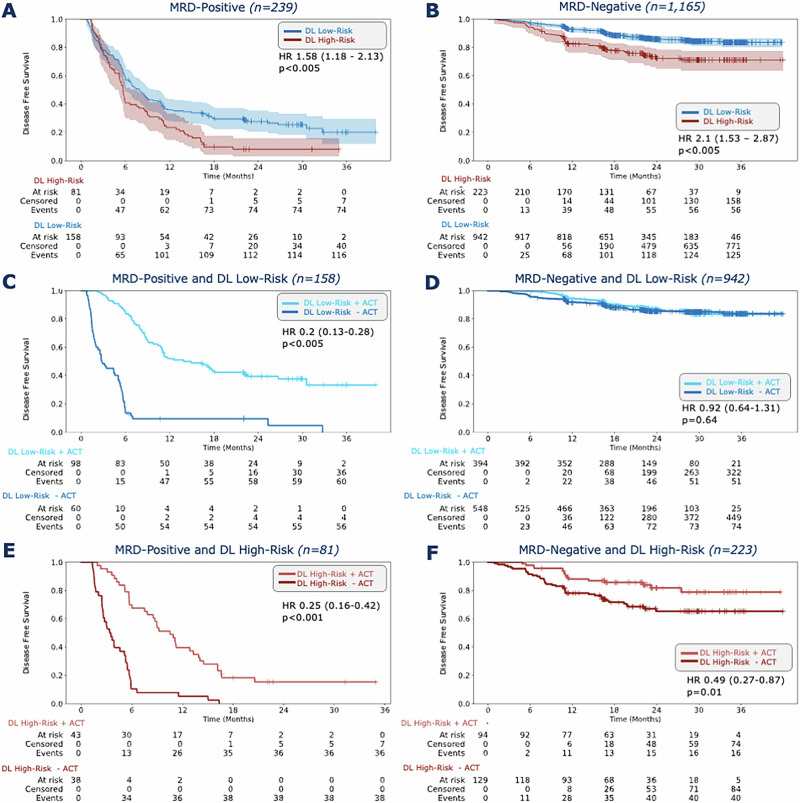
Although surgical resection is the standard therapy for stage II/III colorectal cancer, recurrence rates exceed 30%. Circulating tumor DNA (ctNDA) detects molecular residual disease (MRD), but lacks spatial and tumor microenvironment information. Here, we develop a deep learning (DL) model to predict disease-free survival from hematoxylin & eosin stained whole slide images in stage II-IV colorectal cancer. The model is trained on the DACHS cohort (n = 1766) and validated on the GALAXY cohort (n = 1404). In GALAXY, the DL model categorizes 304 patients as DL high-risk and 1100 as low-risk (HR 2.31; p < 0.005). Combining DL scores with MRD status improves prognostic stratification in both MRD-positive (HR 1.58; p < 0.005) and MRD-negative groups (HR 2.1; p < 0.005). Notably, MRD-negative patients predicted as DL high-risk benefit from adjuvant chemotherapy (HR 0.49; p = 0.01) vs. DL low-risk (HR = 0.92; p = 0.64). Combining ctDNA with DL-based histology analysis significantly improves risk stratification, with the potential to improve follow-up and personalized adjuvant therapy decisions.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: C.M.L.L reports honoraria from AstraZeneca. H.B reports research funding from Ono Pharmaceutical and honoraria from Ono Pharmaceutical, Eli Lilly Japan, and Taiho Pharmaceutical. T.M reports honoraria from Chugai, AstraZeneca, and Miyarisan. S.M reports honoraria from Taiho Pharmaceutical Co., Ltd., Chugai Pharmaceutical Co., Ltd., and Eli Lilly CO, Ltd. D.K reports honoraria from Takeda, Chugai, Lilly, MSD, Ono, Seagen, Guardant Health, Eisai, Taiho, Bristol Myers Squibb, Daiichi-Sankyo, Pfizer, Merckbiopharma, and Sysmex: research funding from Ono, MSD, Novartis, Servier, Janssen, IQVIA, Syneoshealth, CIMIC, and Cimicshiftzero. H.T reports speakers’ bureau from MSD K.K, Merck Biopharma, Takeda, Taiho, Lilly Japan, Bristol-Myers Squibb Japan, Chugai Pharmaceutical, Ono Yakuhin, Amgen; research funding from Takeda, Daiichi Sankyo. I.T reports speakers’ bureau from Medtronic, Johnson &Johnson, Intuitive, Medicaroid, Eli Lilly and research funding from Medtronic, sysmex. S.F has received honoraria from MSD and BMS. T.K reports nothing to declare. E.O reports speakers’ bureau from Chugai Pharmaceutical Co., Ltd., Bristol Meyers, Ono Pharmaceutical Co., Ltd., Eli Lilly, Takeda Pharmaceutical Co., Ltd.; research funding from Guardant Health, Inc.; advisory role from Glaxosmithkline plc. Y.N reports advisory role from Guardant Health Pte Ltd., Natera, Inc., Roche Ltd., Seagen, Inc., Premo Partners, Inc., Daiichi Sankyo Co., Ltd., Takeda Pharmaceutical Co., Ltd., Exact Sciences Corporation, and Gilead Sciences, Inc.; speakers’ bureau from Guardant Health Pte Ltd., MSD K.K., Eisai Co., Ltd., Zeria Pharmaceutical Co., Ltd., Miyarisan Pharmaceutical Co., Ltd., Merck Biopharma Co., Ltd., CareNet, Inc., Hisamitsu Pharmaceutical Co., Inc., Taiho Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd., Chugai Pharmaceutical Co., Ltd., and Becton, Dickinson and Company, Guardant Health Japan Corp; research funding from Seagen,Inc., Genomedia Inc., Guardant Health AMEA, Inc., Guardant Health, Inc., Tempus Labs, Inc., Roche Diagnostics K.K., Daiichi Sankyo Co., Ltd., and Chugai Pharmaceutical Co., Ltd. T.Y.o reports honoraria from Taiho, Chugai, Eli Lilly, Merck, Bayer Yakuhin, Ono and MSD, and research funding from Ono, Sanofi, Daiichi Sankyo, Parexel, Pfizer, Taiho, MSD, Amgen, Genomedia, Sysmex, Chugai and Nippon Boehringer Ingelheim. S.S. The remaining authors declare no competing interests. J.N.K declares consulting services for Owkin, France; DoMore Diagnostics, Norway; Panakeia, UK; Scailyte, Switzerland; Mindpeak, Germany; and MultiplexDx, Slovakia. Furthermore, he holds shares in StratifAI GmbH, Germany, has received a research grant by GSK, and has received honoraria by AstraZeneca, Bayer, Eisai, Janssen, MSD, BMS, Roche, Pfizer and Fresenius. All the other authors report nothing to declare.
Figures

References
-
- Siegel, R. L., Giaquinto, A. N. & Jemal, A. Cancer statistics, 2024. CA Cancer J. Clin.74, 12–49 (2024). - PubMed
-
- Kanemitsu, Y. et al. Hepatectomy followed by mFOLFOX6 versus hepatectomy alone for liver-only metastatic colorectal cancer (JCOG0603): a phase II or III randomized controlled trial. J. Clin. Oncol.39, 3789–3799 (2021). - PubMed
-
- Oki, E. et al. Recurrence monitoring using ctDNA in patients with metastatic colorectal cancer: COSMOS-CRC-03 and AURORA studies. ESMO Gastrointest. Oncol.3, 100034 (2024).
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
