

Pediatric external hemorrhoids: clinical characteristics and outcomes of conservative treatment versus injection sclerotherapy
- PMID: 40813828
- PMCID: PMC12354542
- DOI: 10.1007/s00431-025-06392-2
Pediatric external hemorrhoids: clinical characteristics and outcomes of conservative treatment versus injection sclerotherapy
Abstract
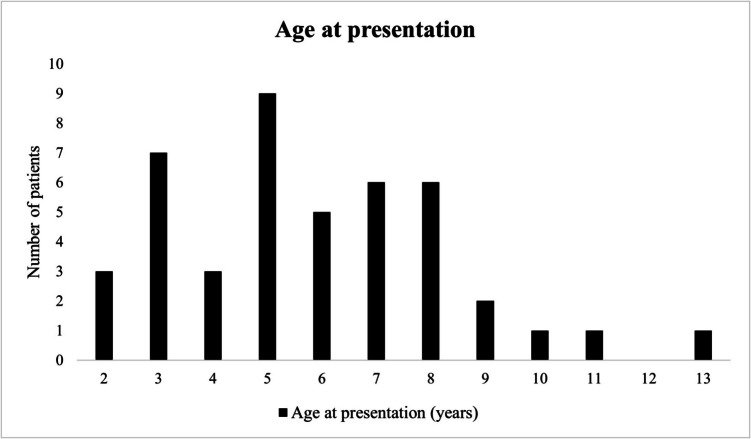
Pediatric external hemorrhoids are rare and often misdiagnosed. This study assesses clinical presentation, risk factors, and treatment outcomes, comparing conservative management with injection sclerotherapy. A retrospective cohort study (2007-2024) was conducted at a tertiary pediatric hospital, including pediatric patients treated with conservative therapy (watchful waiting) or injection sclerotherapy for external hemorrhoids. Data from medical records were analyzed for patient history, presentation, treatment outcomes, and complications. Forty-four patients (86.4% male) were included. Mean age at symptom onset and presentation was respectively 4.0 (range 0-11) and 5.8 (range 2-13) years, with a median diagnostic delay of 20.5 months. All reported anal protrusion/swelling during/after defecation, though this was only visible on examination in 11.4%; diagnosis was otherwise based on parent-provided photographs (63.6%) or reference images (25.0%). Additional symptoms included pain (45.5%), bleeding (18.2%), anal itching (13.6%), anxiety (9.1%) and tenesmus (6.8%). Thirty-one patients (70.5%) underwent injection sclerotherapy, with a 69.2% success rate after one, and 90.3% after two injections. Thirteen patients (29.5%) were treated conservatively with watchful waiting, with symptoms resolving within one year, although the lesion(s) persisted. Skin erosion occurred in 35.5% of patients treated with injection sclerotherapy, leading to constipation and defecation anxiety in 9.1% of patients.
Conclusion: Pediatric external hemorrhoids present as anal protrusion/swelling, often accompanied by anorectal pain. Diagnosis is often delayed due to its intermittent nature. Parent-provided photographs can confirm diagnosis. Both conservative management and injection sclerotherapy are viable treatments; injection sclerotherapy offers a definitive resolution but carries risks of relapse and complications.
What is known: • Pediatric external hemorrhoids are often misdiagnosed and mismanaged.
What is new: • Due to the intermittent nature of external hemorrhoids, diagnosis is often delayed, making parent-provided photographs highly valuable for accurate assessment. • Both conservative management and injection sclerotherapy are viable treatments. • Injection sclerotherapy carries risks of relapse and complications.
Keywords: Conservative management; Injection sclerotherapy; Parent-provided photographs; Pediatric external hemorrhoids.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This study was performed in line with the principles of the Declaration of Helsinki. The study was ethically evaluated by the ethical review board of the Amsterdam UMC and deemed not applicable to the Medical Research Involving Human Subjects Act (WMO) (ref. 2024.0004, July 24, 2024). Informed consent was obtained from all included individual patients (or parents). The authors affirm that patients provided informed consent for publication of the images in Figs. 1 and 2. Competing interests: The authors declare no competing interests.
Figures



References
-
- Stites T, Lund DP (2007) Common anorectal problems. Semin Pediatr Surg 16:71–78. 10.1053/j.sempedsurg.2006.10.010 - PubMed
-
- Dimopoulou K, Dimopoulou A, Dimopoulou D, Zavras N, Fessatou S (2022) Benign anorectal disease in children: what do we know? Arch Pediatr 29:171–176. 10.1016/j.arcped.2022.01.015 - PubMed
-
- Haas PA, Fox TA Jr, Haas GP (1984) The pathogenesis of hemorrhoids. Dis Colon Rectum 27:442–450. 10.1007/BF02555533 - PubMed
-
- Orkin BA, Schwartz AM, Orkin M (1999) Hemorrhoids: what the dermatologist should know. J Am Acad Dermatol 41:449–456. 10.1016/s0190-9622(99)70120-9 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
