

Kidney Disease: Improving Global Outcomes Summit Recommendations on Implementation of Diabetes Management in CKD: From Primary to Data-Driven Collaborative Care
- PMID: 40814615
- PMCID: PMC12348363
- DOI: 10.1016/j.ekir.2025.06.010
Kidney Disease: Improving Global Outcomes Summit Recommendations on Implementation of Diabetes Management in CKD: From Primary to Data-Driven Collaborative Care
Abstract
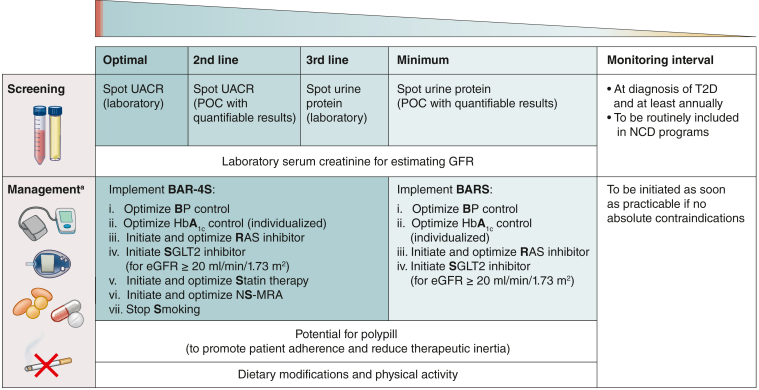
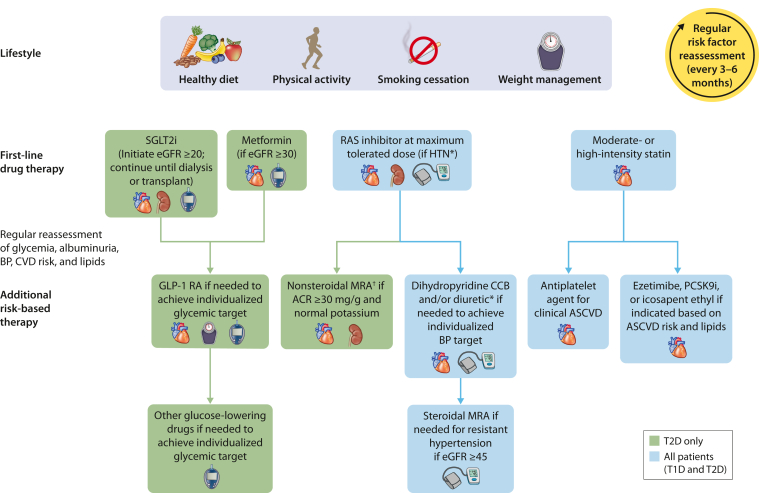
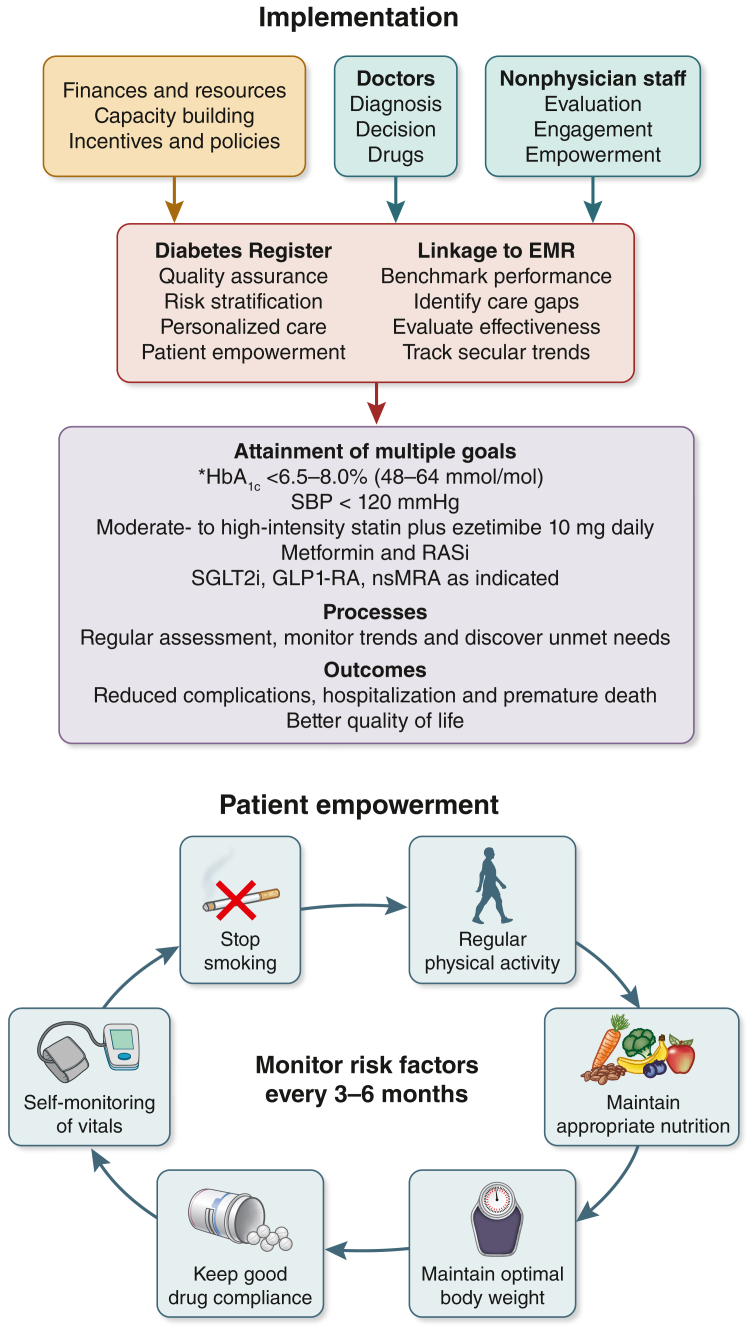
Type 2 diabetes and chronic kidney disease (CKD) are preventable and treatable. Their silent and progressive clinical course calls for structured assessment with timely feedback to patients and care providers for activating decision-making. Apart from CKD, patients with diabetes can have complications affecting multiple organs, notably the cardiovascular system, eyes, and feet. International practice guidelines recommend annual assessment of the eyes, feet, blood, and urine to detect silent complications and measure cardiovascular-kidney-metabolic (CKM) risk factors to ensure early intervention, including treatment to multiple targets and use of organ-protective drugs. In this report, we highlight the barriers and gaps in the implementation of practice guidelines in managing diabetes in CKD with proposed solutions to overcome such barriers. By improving the practice environment and workflow, nurses can be trained to perform protocol-guided evaluation under medical supervision. The systematic data collection enables physicians to make timely decisions, including drug prescriptions and referrals to other specialists to promote collaborative care, whereas nurses can use the personalized data to empower patient self-management and improve health literacy. This ongoing data collection will form a register to align payers, providers, and patients in delivering data-driven and value-based care with the creation of real-world evidence to verify treatment effectiveness and identify care gaps while providing on-the-job training. When accompanied by a biobank, the ongoing collection and analysis of this multidimensional data will refine diagnosis, classification, prognosis, and treatment in pursuit of precision medicine.
Keywords: CKD; KDIGO; collaborative care; diabetes; primary care; specialist care.
© 2025 Published by Elsevier, Inc., on behalf of the International Society of Nephrology.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
