

Treatment With Avacopan in ANCA-Associated Vasculitis With Kidney Involvement
- PMID: 40814647
- PMCID: PMC12348124
- DOI: 10.1016/j.ekir.2025.05.041
Treatment With Avacopan in ANCA-Associated Vasculitis With Kidney Involvement
Abstract
Introduction: Kidney disease impacts long-term outcomes of patients with granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA). This post hoc analysis evaluated the effect of avacopan in a subgroup of patients with GPA or MPA and kidney involvement at baseline from the ADVOCATE trial.
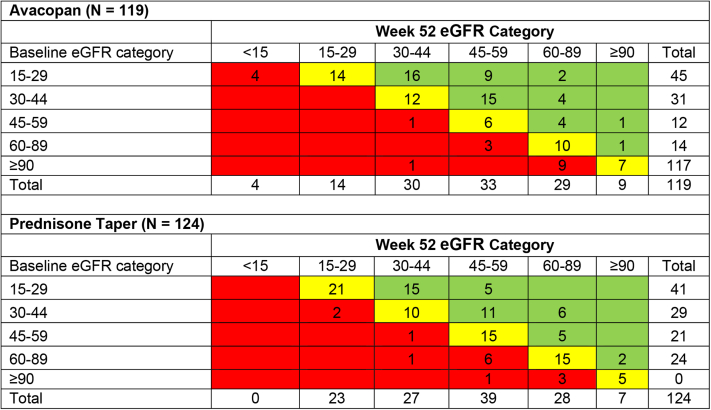
Methods: The analysis included a study population of 268 patients (of 330 patients, 81.2%). Key efficacy outcomes were remission at week 26, sustained remission at week 52, and relapse after remission through week 52. Changes in estimated glomerular filtration rate (eGFR) were analyzed overall and stratified by baseline eGFR categories (≥ 90, 60-89, 45-59, 30-44, and 15-29 ml/min per 1.73 m2). Additional outcomes were changes in albuminuria and hematuria, glucocorticoid (GC) use, glucocorticoid toxicity index (GTI), and safety.
Results: Remission at week 26 and sustained remission at week 52, respectively, were respectively achieved by 99 of 134 (73.9%) and 91 of 134 (67.9%) patients in the avacopan group and 95 of 134 (70.9%) and 76 of 134 (56.7%) in the prednisone taper group. Relapse rate after remission was lower in the avacopan than in the prednisone taper group (9.4% vs. 20.9%; hazard ratio [95% confidence interval, CI]: 0.43 [0.22-0.85]). Recovery of kidney function, speed of reduction in albuminuria and hematuria, and changes in GTI favored the avacopan group. No new safety issues were reported for this subset of patients.
Conclusion: In patients with GPA or MPA with kidney involvement, treatment with an avacopan regimen compared with a prednisone taper regimen achieved similar rates of remission, improved recovery of kidney function, led to faster reduction in albuminuria and hematuria, and lowered GC-related toxicity, with an acceptable safety profile.
Keywords: ANCA; complement; granulomatosis with polyangiitis (GPA); hematuria; microscopic polyangiitis (MPA); proteinuria.
© 2025 International Society of Nephrology. Published by Elsevier Inc.
Figures




References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
