

Longitudinal assessment of migraine burden in resistant and refractory migraine - Data from the prospective REFINE study
- PMID: 40817153
- PMCID: PMC12355733
- DOI: 10.1186/s10194-025-02126-9
Longitudinal assessment of migraine burden in resistant and refractory migraine - Data from the prospective REFINE study
Abstract
Background: Some individuals with migraine fail to respond adequately to preventive treatments, bearing most of migraine burden. The European Headache Federation (EHF) classifies these individuals into resistant migraine (ResM) or refractory migraine (RefM) according to treatment failures, debilitating headache days, and disease duration. We investigated the evolution of these categories over six months in patients treated at tertiary headache centers and whether they accurately reflect disability and burden.
Methods: Participants from the multicenter, prospective REFINE study were classified into three categories of treatment responsiveness, namely RefM, ResM, and non-refractory non-resistant migraine (NRNRM). The primary objective was to determine the trajectories of category changes over six months. Secondary outcomes included changes in the 6-item Headache Impact Test (HIT-6), Headache-Attributed Lost Time (HALT), and Hospital Anxiety and Depression Scale (HADS-A and HADS-D) scores.
Results: Overall, 489 participants were included with a median age of 45 years (IQR = 36-53); 389 participants (79.7%) were female; 256 (52.4%) had NRNRM, 178 (36.4%) ResM, and 55 (11.2%) RefM. At follow-up, 200/256 (78.1%) NRNRM remained stable, while 56/256 (21.9%) progressed to ResM. Among those with ResM, 98/178 (55.1%) remained stable, 72/178 (40.5%) improved to NRNRM, and 8/178 (4.5%) worsened to RefM. Among participants with RefM, 37/55 (67.3%) remained stable, while 18/55 (32.7%) improved to NRNRM. Participants with RefM and ResM presented significantly higher scores at baseline than those with NRNRM. Over time, HIT-6, HALT, and HADS-A scores improved substantially in the overall cohort (p < 0.001, p < 0.001, and p = 0.006, respectively). Improvements were observed in participants with ResM across all scores and HIT-6 and HALT for NRNRM, but no improvement was noted in participants with RefM.
Conclusions: Over six months, ~ 40% of ResM and ~ 30% of RefM individuals improved to NRNRM, while ~ 20% of NRNRM developed treatment resistance after receiving care in tertiary headache centers. Participants with ResM had a better prognosis than those with RefM. While both ResM and RefM reflect high migraine disability burden, they might present relevant differences in their management and prognosis.
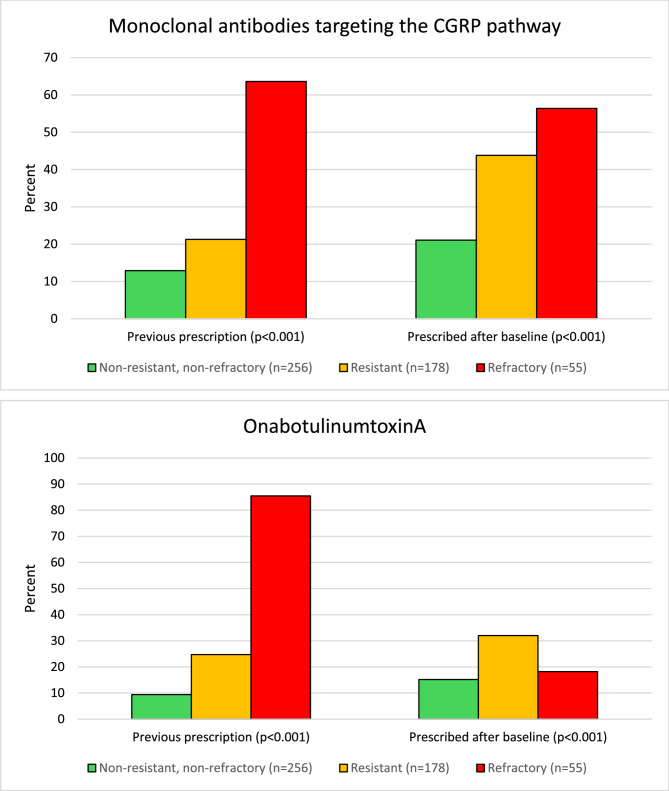
Keywords: Anti-CGRP; Chronic migraine; Disability; Gepants; Headache; Intractable; Monoclonal antibodies; Validation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Consent for publication: Participants or their authorized representatives provided written informed consent. Competing interests: PM serves as the Editor-in-Chief of The Journal of Headache and Pain and SN Comprehensive Clinical Medicine. M.W-P is a member of the Editorial Board of The Journal of Headache and Pain. RO reports personal fees or non-financial support from AbbVie, Bayer, Eli Lilly, Lundbeck, Novartis, Organon, Pfizer, and Teva; he is an Editorial Board Member of The Journal of Headache and Pain, Confinia Cephalalgica, and Associate Editor for Frontiers in Neurology and Arquivos de Neuropsiquiatria. PP-R reports in the last 36 months, fees as a consultant and speaker for: AbbVie, Dr. Reddy’s, Eli Lilly, Lundbeck, Medscape, Novartis, Organon, Pfizer and Teva. Her research group has received research grants from AbbVie, Novartis and Teva; as well as, InstitutoSalud Carlos III, EraNet Neuron, European Regional Development Fund (001-P-001682) under theframework of the FEDER Operative Programme for Catalunya 2014-2020 - RIS3CAT; has receivedfunding for clinical trials from AbbVie, Amgen, Biohaven, Eli Lilly, Lundbeck, Novartis, Pfizer Teva. SS reports personal fees as speaker or advisor from Abbott, Allergan-Abbvie, AstraZeneca, Bayer, Boehringer, Eli Lilly, Lundbeck, Pfizer, and Teva; she received research grants from Novartis and Uriach; she is President of the European Stroke Organisation, Editor-in-Chief of Cephalalgia and Cephalalgia Reports, and Assistant Editor for Stroke. DM has received fees and travel grants from AbbVie, Bristol Myers Squibb, Cross Pharma, Eli Lilly, Genesis Pharma, Haleon, Merck, Lundbeck, Novartis, Orion, Roche, Pfizer, Viatris, AstraZeneca, and Teva Pharmaceuticals; has participated in clinical trials for Amgen, Eli Lily, Lundberg, Novartis, Pfizer, and Teva Pharmaceuticals, as principal investigator; is president of the Hellenic Headache Society; is a member of the Management Group of the Headache Scientific Panel and of the Coordinating panel for the Functional Neurological Disorders at the European Academy of Neurology; and a past-President of the European Headache Federation. AO reports receiving personal fees as a speaker or advisor from AbbVie, Eli Lilly, TEVA, Pfizer, Organon, Ali Raif, İlko, and Neutec. She is a board member of IHS. She is the current president of the Global Migraine and Pain Society and MENAA Headache Society. She serves as a guest editor or reviewer for several Journals, including Cephalalgia, Cephalalgia Reports, TJHP, BMC Neurology, Headache, and Frontiers in Neurology. FV received travel grants, honoraria for advisory board, speaker panels, or clinical investigation studies from Allergan/AbbVie, Angelini, Eli Lilly, Lundbeck, Novartis, Pfizer, and Teva Pharmaceuticals; he serves as Specialty Chief Editor of Frontiers in Neurology Headache and Neurogenic Pain section. MB previously received sponsorship, financial support, fees from: Abbott Laboratories, AbbVie Inc, Allergan Inc, Berlin-Chemie AG (Menarini Group), Boehringer Ingelheim Pharma GmbH, Desitin Arzneimittel GmbH, EV3, Gedeon Richter Ltd, GlaxoSmithKline, KBM Pharma Ltd., H. Lundbeck A/S, Novartis Pharma Services Inc, Nycomed SEFA, Orion Pharma, Pfizer Inc, Sanofi-Aventis, Sandoz d.d., Scanmed Group, Solvay Pharmaceuticals, Teva Pharmaceutical Industries Ltd./Sicor Biotech UAB, Zentiva International. Ethical approval and consent to participate: was obtained from the Institutional Review Board and/or relevant Ethics Committees at all participating centers (protocol number from coordinating center: 45/2020-21). Participants or their authorized representatives provided written informed consent.
Figures




References
-
- Global incidence (2024) prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the global burden of disease study 2021. Lancet 403:2133–2161 - PMC - PubMed
-
- Ferrari MD, Goadsby PJ, Burstein R et al (2022) Migraine Nat Rev Dis Primers 8:2 - PubMed
-
- Edvinsson L, Haanes KA, Warfvinge K, Krause DN (2018) CGRP as the target of new migraine therapies - successful translation from bench to clinic. Nat Rev Neurol 14:338–350 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
