

The physical therapy efficacy index and chart: a stimulus for value-based healthcare using real-world data
- PMID: 40817216
- PMCID: PMC12355830
- DOI: 10.1186/s12913-025-13092-y
The physical therapy efficacy index and chart: a stimulus for value-based healthcare using real-world data
Abstract
Background: Health care costs are rising rapidly in Western societies. Understanding the benefits and costs of care is crucial to maintaining or improving existing health care systems. We propose an instrument that provides a clear overview of both the costs and returns of a treatment to improve the quality of care while keeping the costs affordable.
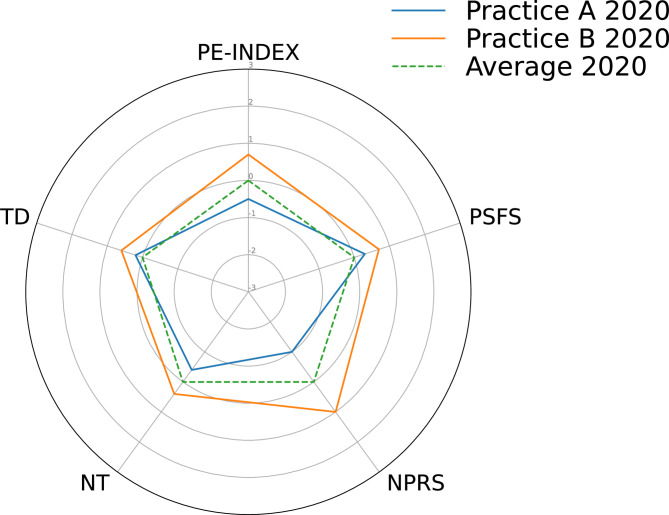
Methods: First, a general value-based healthcare concept was developed as an efficacy index. Second, a Physiotherapy-specific Efficacy Index (PE-Index) for musculoskeletal disorders was formulated based on pain and functional improvement, treatments, and episode duration. The PE-Index discriminative value was assessed using a linear mixed model with physiotherapy practices as a random effect in real-world data from a national registry. Variation attributed to practices was quantified by an intraclass correlation coefficient. Separate linear mixed models and a radar plot (PE-Graph) visualized individual PE-Index components. Lastly, stakeholders evaluated the PE-Index and PE-Graph for internal quality improvement and external transparency through surveys and advisory board meetings.
Results: In total, 95.805 episodes treated in 370 practices were included in the linear mixed models. The PE-Index demonstrated an adequate discriminative ability with an ICC of 0.118. Stakeholders agree that the PE-Index and the PE-Chart are appropriate for improvement of quality of care and enhancing the current system for external transparency. Nevertheless, because of concerns about a too hasty implementation and the risk of strategic gaming, both were not considered suitable for external transparency right now.
Conclusions: The PE-Index and PE-Graph are adequate instruments to discriminate between practices and can be used for internal quality improvement, however, are not yet suitable for external transparency purposes.
Keywords: Clinimetrics; Learing Health System; Organisation of Care; Real World Data; Value-Based Healthcare.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The data were collected by physical therapists during standard care through their electronic health records and classified using a four-digit coding system based on body location and pathology [8] (Table A1 in the appendix). Under Dutch law, the use of electronic health records for research purposes is permitted under certain conditions. When these conditions are met, neither obtaining informed consent from patients nor approval by a medical ethics committee is required for observational studies containing no directly identifiable data (art. 24 GDPR Implementation Act jo art. 9.2 sub j GDPR; Dutch Civil Law, Article 7:458). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- CBS Statistics Netherlands. Centraal Bureau voor de Statistiek. 2023 [cited 2023 Dec 27]. Zorguitgaven; kerncijfers. Available from: https://www.cbs.nl/nl-nl/cijfers/detail/84047NED?dl=926E6
-
- Fatoye F, Wright JM, Gebrye T. Cost-effectiveness of physiotherapeutic interventions for low back pain: a systematic review. Physiotherapy. 2020;108:98–107. - PubMed
-
- Porter ME, Teisberg EO. Redefining Health Care: Creating Value-Based Competition on Results. Boston: Harvard Business School Press; 2006.
-
- Hartrick CT. A four-category verbal rating scale (VRS-4), an 11-point numeric rating scale (NRS-11), and a 100-mm visual analog scale (VAS) were compared in the assessment of acute pain after oral surgery. Clin J Pain. 2001;17(1):104–5. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
