

Dynamic brain-heart interaction in sleep characterized by variational phase-amplitude coupling framework
- PMID: 40818995
- PMCID: PMC12357881
- DOI: 10.1038/s42003-025-08685-6
Dynamic brain-heart interaction in sleep characterized by variational phase-amplitude coupling framework
Abstract
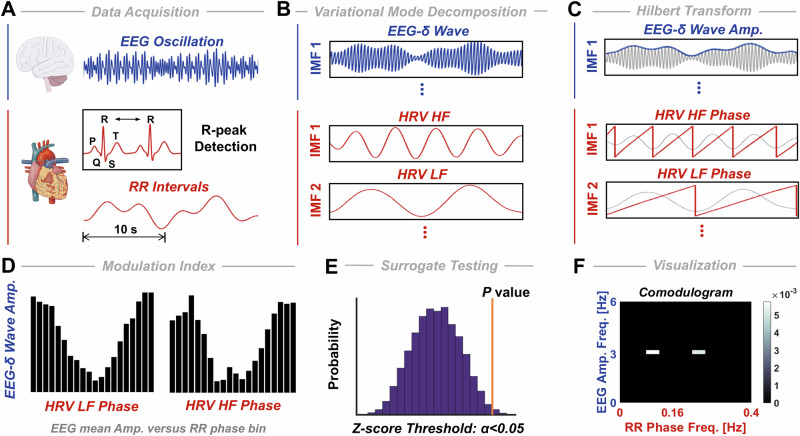
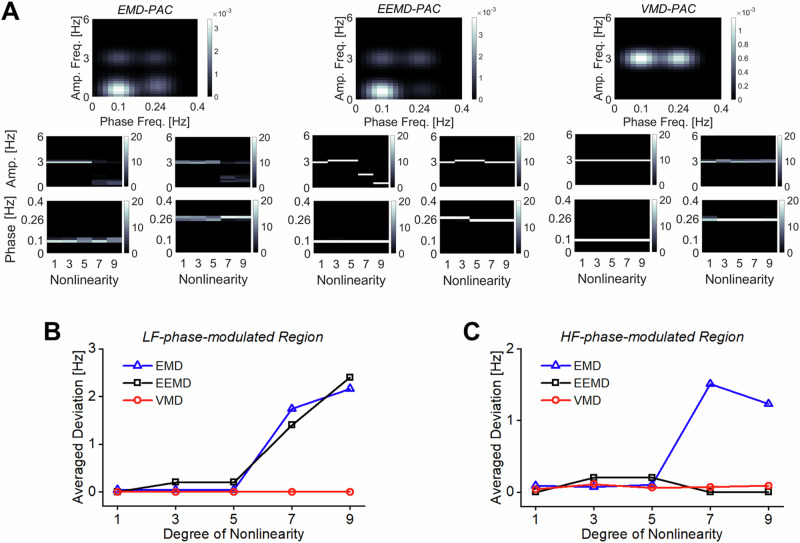
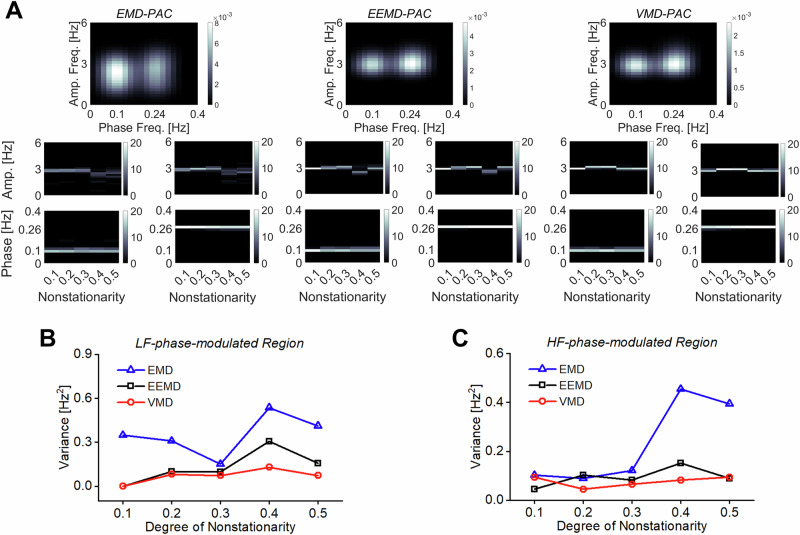
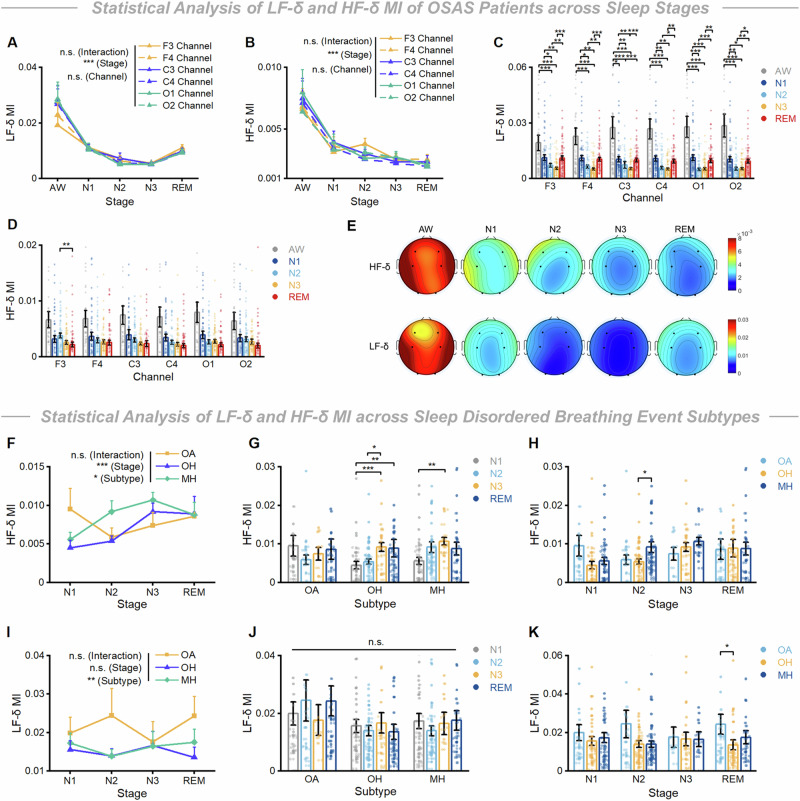
Sleep is a complex physiological state characterized by synchronized cortical and cardiac oscillations, which reflect dynamic communication and interaction between the central (CNS) and autonomic (ANS) nervous systems, crucial for maintaining homeostasis and overall health. However, the dynamic interplay between CNS and ANS rhythmicities in sleep remains unclear. Here, we present a variational phase-amplitude coupling framework that associates frequency modulations of the electroencephalogram and cardiac R-peak intervals across sleep dynamics. We validate the robustness of our method on spurious couplings by nonlinear or nonstationary simulations. Moreover, delta-range slow cortical oscillations exhibit robust coupling with both the low- (HRV-LF) and high-frequency (HRV-HF) constituents of RR-interval heart-rate variability, thereby constituting a cardinal electrophysiological signature of ANS-CNS modulation. Furthermore, we highlight the significance of the "decoupling phenomenon" in a transitional period from wake to sleep for sleep preparation, and discover stronger couplings between the HRV-LF component and EEG-δ wave, and weaker couplings between the HRV-HF component and EEG-δ activity for obstructive sleep apnea (OSA) patients compared to healthy individuals, and finally uncover the key patterns of brain-heart interaction in both healthy cohorts and OSA patients during sleep.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures



Similar articles
-
Heart rate variability analysis in comorbid insomnia and sleep apnea (COMISA).Sci Rep. 2025 May 21;15(1):17574. doi: 10.1038/s41598-025-02541-7. Sci Rep. 2025. PMID: 40399494 Free PMC article.
-
Heart rate variability analysis in obstructive sleep apnea patients with daytime sleepiness.Sleep. 2024 Jun 13;47(6):zsae075. doi: 10.1093/sleep/zsae075. Sleep. 2024. PMID: 38531670 Free PMC article.
-
Study of heart rate variability in healthy humans as a function of age: considerations on the contribution of the autonomic nervous system and the role of the sinoatrial node.Front Med (Lausanne). 2025 Aug 7;12:1597299. doi: 10.3389/fmed.2025.1597299. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40852364 Free PMC article.
-
A systematic review and meta-analysis of heart rate variability in epilepsy and antiepileptic drugs.Epilepsia. 2012 Feb;53(2):272-82. doi: 10.1111/j.1528-1167.2011.03361.x. Epub 2012 Jan 5. Epilepsia. 2012. PMID: 22221253
-
The Impact on Autonomic Nervous System Activity during and Following Exercise in Adults: A Meta-Regression Study and Trial Sequential Analysis.Medicina (Kaunas). 2024 Jul 28;60(8):1223. doi: 10.3390/medicina60081223. Medicina (Kaunas). 2024. PMID: 39202504 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
