

Incidence and risk factors of acute kidney injury after abdominal surgery: a systematic review and meta-analysis
- PMID: 40819346
- PMCID: PMC12360056
- DOI: 10.1080/07853890.2025.2547324
Incidence and risk factors of acute kidney injury after abdominal surgery: a systematic review and meta-analysis
Abstract
Objective: To determine the incidence of acute kidney injury (AKI) following abdominal surgery, assess its outcome associations, and identify factors associated with postoperative AKI development.
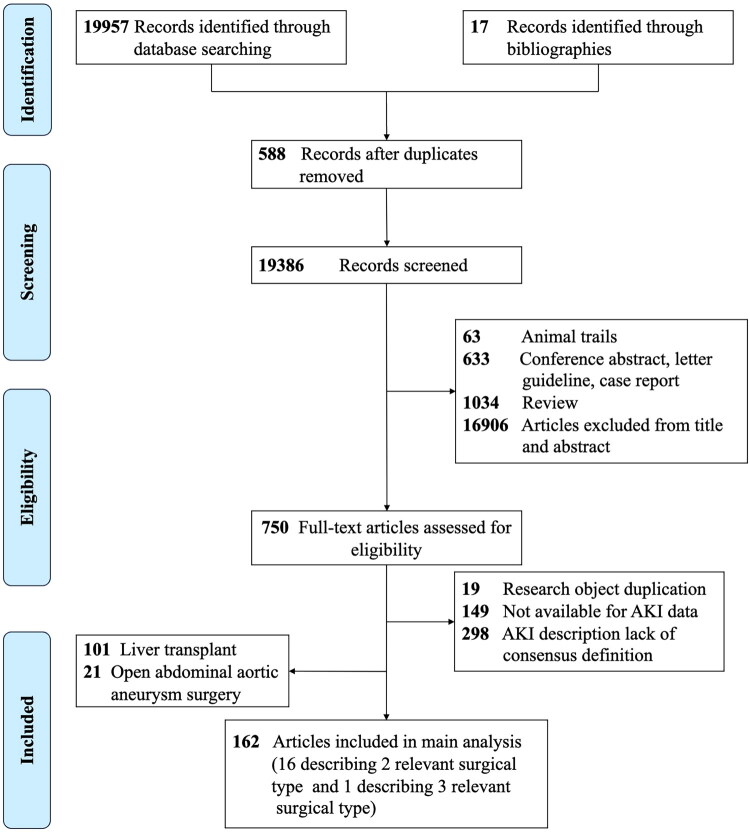
Methods: We performed a systematic search of PubMed, Embase, and Cochrane Database of Systematic Reviews, from January 2004, to December 2024. We included studies reporting AKI based on consensus criteria (RIFLE, AKIN, or KDIGO) in adult abdominal surgery patients.
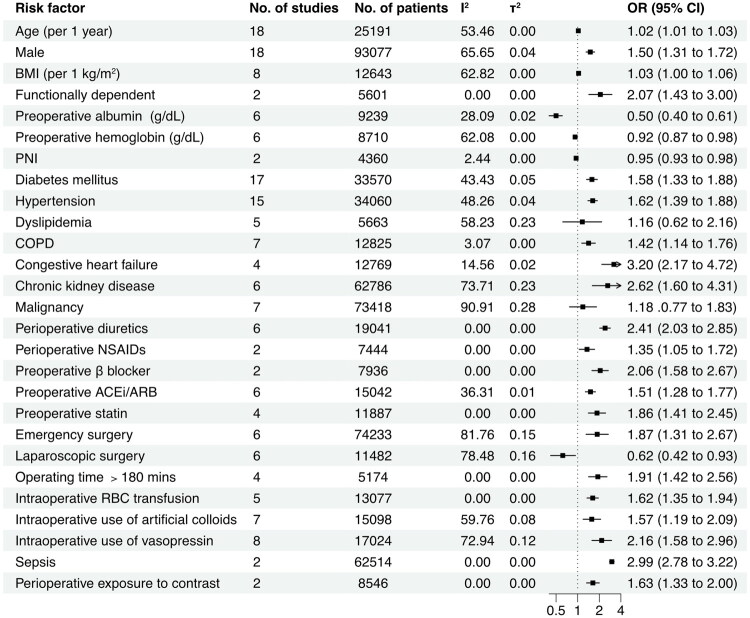
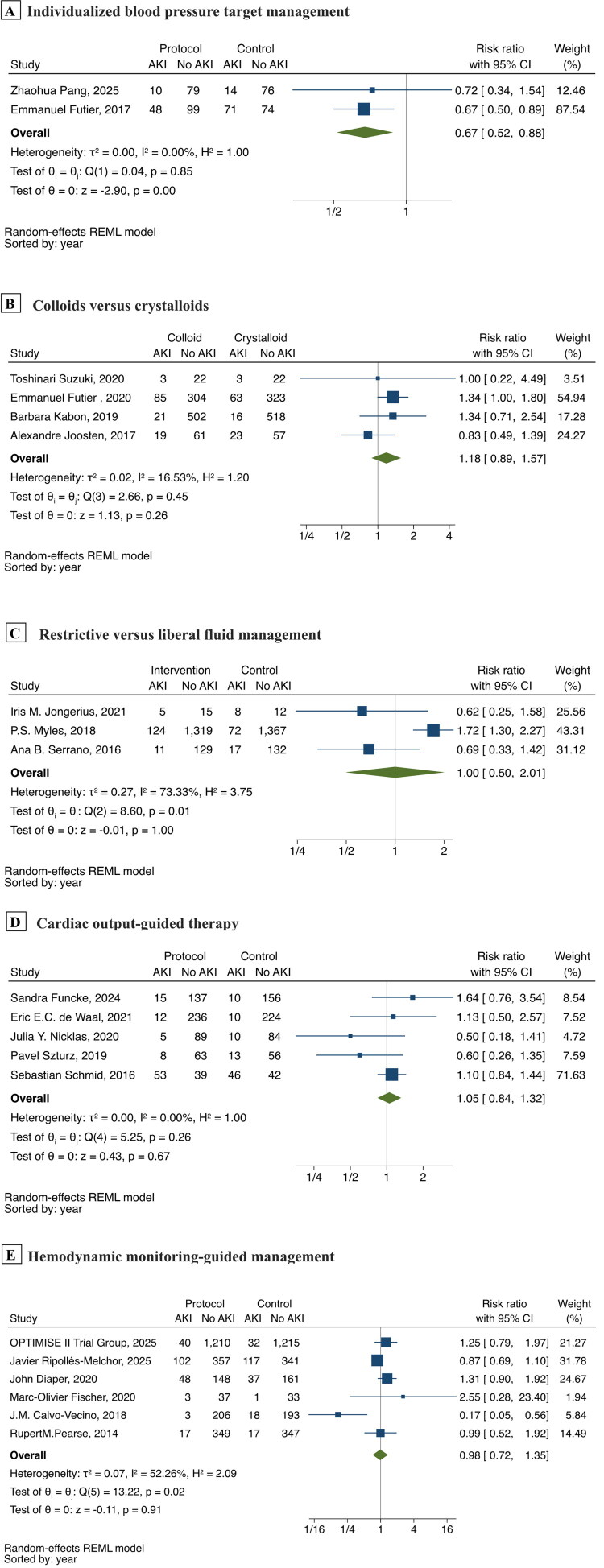
Results: A total of 162 studies (675361 patients) were included. The pooled AKI incidence was 16% (95% CI: 14-17%), with significant variation by surgical procedure. Meta-analysis showed AKI was significantly associated with increased short-term mortality (risk ratio [RR], 6.46; 95% CI: 4.63-9.00) and long-term mortality (RR, 6.36; 95% CI: 3.32-12.16). Mortality risk demonstrated stage-dependent increase, with RR of 2.74 (95%CI: 1.77-4.24), 8.01 (95%CI: 3.18-20.18), and 15.73 (95%CI: 5.52-44.81) for AKI stages 1, 2, and 3, respectively. AKI was associated with prolonged hospital stay (weighted mean difference 4.72 days; 95%CI: 3.43-6.02), also showeing stage-dependent increase of 5.03, 11.16, and 14.46 days for stages 1, 2, and 3, respectively. Twenty-five risk factors were associated with AKI. Meta-analysis of randomized controlled trials revealed that individualized blood pressure target management significantly reduced AKI incidence (RR, 0.67; 95% CI: 0.52-0.88).
Conclusions: AKI remains a common and important complication after abdominal surgery, with severity showing a graded association with mortality and hospital stay. Individualized blood pressure management demonstrates promise in AKI prevention.
Registration: PROSPERO CRD42022304083.
Keywords: Acute kidney injury; abdominal surgery; incidence; risk factor; systematic review.
Plain language summary
The incidence of postoperative AKI after abdominal surgery is 16% (95% CI: 14–17%), varying by specific abdominal surgical procedure but not significantly different over time or by consensus definition.AKI severity shows a strong graded association with both short-term and long-term mortality, as well as prolonged hospital stays.Twenty-five factors were identified, providing valuable information for clinical risk assessment.Meta-analysis of randomized trials reveals that individualized blood pressure target management significantly reduces AKI incidence, while other single perioperative interventions (crystalloids versus colloids, restrictive versus liberal fluid management, cardiac output-guided therapy, hemodynamic monitoring) show no significant protective effects.
Conflict of interest statement
No conflicts of interest to declare.
Figures


Similar articles
-
Fenoldopam for preventing and treating acute kidney injury.Cochrane Database Syst Rev. 2024 Nov 28;11(11):CD012905. doi: 10.1002/14651858.CD012905.pub2. Cochrane Database Syst Rev. 2024. PMID: 39607014
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2020 Jan 9;1(1):CD011535. doi: 10.1002/14651858.CD011535.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Apr 19;4:CD011535. doi: 10.1002/14651858.CD011535.pub4. PMID: 31917873 Free PMC article. Updated.
-
Incidence and associations of acute kidney injury after major abdominal surgery.Intensive Care Med. 2016 Apr;42(4):521-530. doi: 10.1007/s00134-015-4157-7. Epub 2015 Nov 24. Intensive Care Med. 2016. PMID: 26602784
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Continuous positive airway pressure (CPAP) during the postoperative period for prevention of postoperative morbidity and mortality following major abdominal surgery.Cochrane Database Syst Rev. 2014 Aug 1;2014(8):CD008930. doi: 10.1002/14651858.CD008930.pub2. Cochrane Database Syst Rev. 2014. PMID: 25081420 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical