

Long-term survival after multidisciplinary heart team-guided management of complex coronary artery disease
- PMID: 40821489
- PMCID: PMC12351742
- DOI: 10.1080/08998280.2025.2516981
Long-term survival after multidisciplinary heart team-guided management of complex coronary artery disease
Abstract
Objective: Guidelines recommend a multidisciplinary heart team approach for managing complex coronary artery disease (CAD), yet its impact on clinical outcomes and adherence to recommendations is rarely reported.
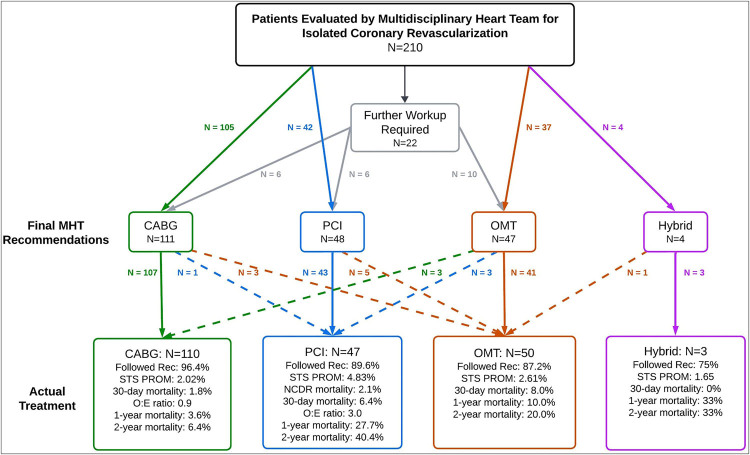
Methods: Between June 2021 and August 2022, 210 high-risk patients with isolated, complex CAD were evaluated at our institution's weekly heart team conference for consideration of coronary artery bypass grafting (CABG), percutaneous coronary intervention (PCI), hybrid PCI/CABG, or optimal medical therapy (OMT). Adherence to recommendations and clinical outcomes, including 30-day, 1-year, and 2-year mortality, were assessed.
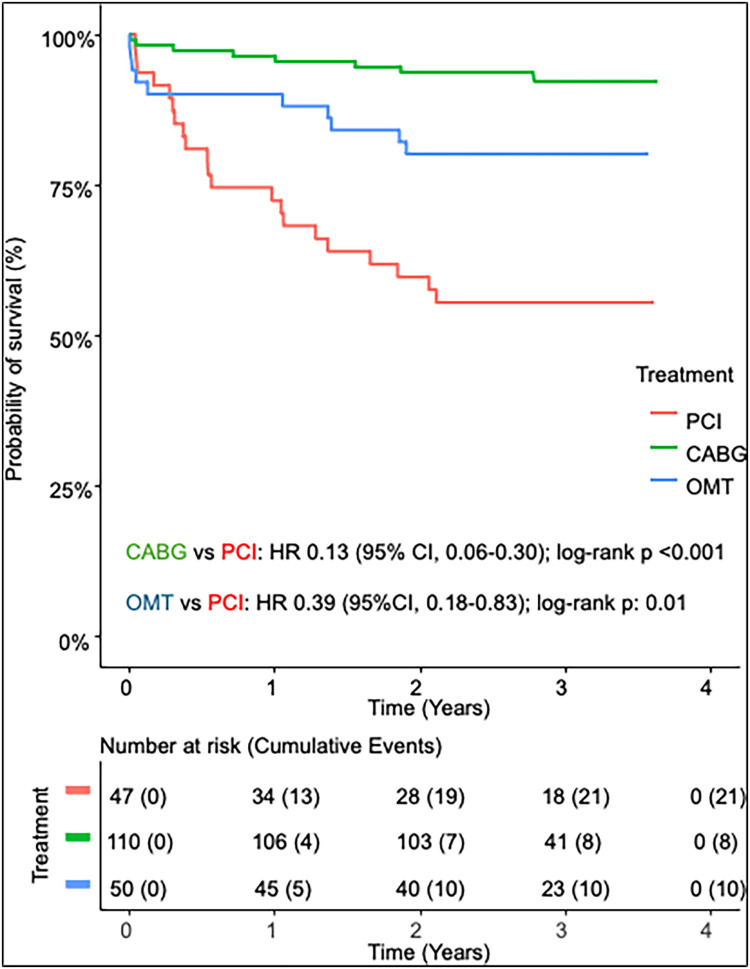
Results: Overall adherence to heart team recommendations was 92%, with 96% adherence for CABG, 90% for PCI, 87% for OMT, and 75% for hybrid PCI/CABG. CABG was the most frequently recommended treatment (53%) and demonstrated the lowest mortality at 1 year (4%) and 2 years (6%) compared with PCI (1 year, 28%; 2 year, 40%) and OMT (1 year, 10%; 2 year, 20%). CABG patients had a lower-than-expected mortality (observed-to-expected ratio 0.9), while PCI was associated with significantly higher mortality (observed-to-expected ratio 3.0).
Conclusion: This single-center multidisciplinary heart team approach for complex CAD offers a collaborative, patient-centered model that facilitates high adherence rates and favorable patient outcomes. These findings highlight the potential benefits of integrating multidisciplinary evaluation and support its implementation into standard practice for high-risk CAD patients.
Keywords: Coronary artery bypass grafting; coronary artery disease; long-term outcomes; multidisciplinary heart team; percutaneous coronary intervention.
Copyright © 2025 Baylor University Medical Center.
Conflict of interest statement
Dr. Potluri: Advisory board member, proctor, and speaker for Medtronic, Boston Scientific, Abbott, and Cordis; proctor and speaker for Edwards Lifesciences, Terumo, and AstraZeneca. Dr. Szerlip: Proctor, speaker, and consultant for Edwards Lifesciences; advisory board member, consultant, and proctor for Abbott Vascular; steering committee member for Medtronic; speaker for Boston Scientific. Dr. Al-Azizi: Proctor and consultant for Edwards Lifesciences; consultant and advisory board member for Medtronic; consultant for Boston Scientific; speaker bureau member. Dr. Harrington: Consultant for Abbott Laboratories and Maquet Cardiovascular; speaker for Artivion, Inc. and Medtronic, Inc.; speaker and advisory board member for Boston Scientific Corporation; speaker and proctor for Edwards Lifesciences Corporation. Dr. Brinkman: Teaching and travel support from Artivion; consultant for Bolton Medical, Inc., Maquet Cardiovascular, Medtronic, Terumo Medical Corporation, and W.L. Gore; advisory board member for Medtronic. Dr. Smith: Grant support recipient from Edwards Lifesciences; speaker honoraria recipient from Edwards Lifesciences, Abbott, and CryoLife. Dr. George: Speaker for Abiomed. Dr. DiMaio: Investment and ownership interests in HeartFlow, Inc. and Spectral MD. The remaining authors have no competing interests to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous