

Vonoprazan and amoxicillin dual therapy versus bismuth-based therapy for Helicobacter pylori eradication: a systematic review and meta-analysis of randomized controlled trials
- PMID: 40821497
- PMCID: PMC12351748
- DOI: 10.1080/08998280.2025.2491964
Vonoprazan and amoxicillin dual therapy versus bismuth-based therapy for Helicobacter pylori eradication: a systematic review and meta-analysis of randomized controlled trials
Abstract
Introduction: Helicobacter pylori infection can cause peptic ulcer disease, chronic gastritis, primary gastric lymphoma, and gastric cancer. Treatment with bismuth-based quadruple therapy is typically the first line of treatment but can be challenging due to increased pill burden and adverse effects, leading to nonadherence to therapy. Recent studies have shown that vonoprazan can be used in combination with amoxicillin as a potential treatment option. We conducted a systematic review and meta-analysis to assess the efficacy and tolerability of vonoprazan-based dual therapy as compared to bismuth-based therapy (BBT).
Methodology: We conducted a comprehensive search of multiple electronic databases including PubMed, Embase, and Cochrane Library to identify randomized controlled studies assessing vonoprazan and amoxicillin (VA) in comparison to BBT for H. pylori treatment in adults >18 years of age. Studies with pediatric populations, written in languages other than English, or without control groups were excluded.
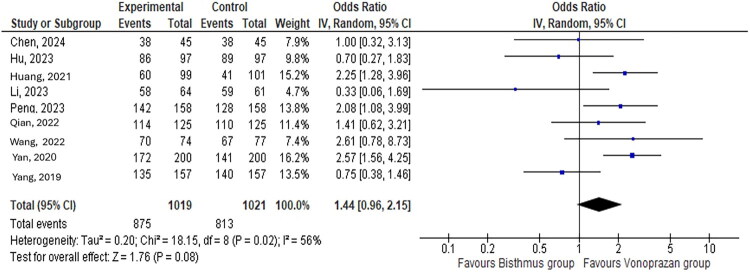
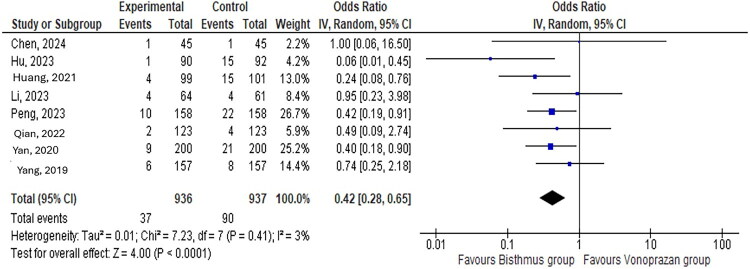
Results: Out of the 1968 citations, 9 studies including 2039 patients were included in the final analysis. There were 463 and 481 men in the VA and the BBT groups, respectively. The mean age ranged from 38.1 to 48.7 years in the VA group and from 38.6 to 46.1 in the BBT group. The VA group had an eradication rate similar to that of the BBT group (odds ratio [OR]: 0.32, 95% confidence interval [CI]: 0.26-0.40; P = 0.08). The VA group had a lower incidence of total adverse events than the BBT group (OR: 0.32, 95% CI: 0.26-0.40; P = 0.0001), including a reduced occurrence of nausea and vomiting (OR: 0.42, 95% CI: 0.28-0.65; P = 0.0001). There was no difference in compliance between the VA and BBT groups (OR: 1.16, 95% CI: 0.76-1.76; P = 0.50).
Conclusion: Our study showed a similar eradication rate of H. pylori but a significantly lower incidence of adverse events in the VA group compared with the BBT group. Our analysis suggests that a VA-based regimen is an acceptable treatment option for H. pylori patients who cannot tolerate BBT.
Keywords: Bismuth; Helicobacter pylori; vonoprazan.
Copyright © 2025 Baylor University Medical Center.
Conflict of interest statement
The authors report no funding or conflicts of interest.
Figures




Similar articles
-
Fourteen-day vonoprazan-amoxicillin dual therapy versus 14-day bismuth-based quadruple therapy for Helicobacter pylori treatment: a randomized clinical trial.Therap Adv Gastroenterol. 2025 Jul 13;18:17562848251354868. doi: 10.1177/17562848251354868. eCollection 2025. Therap Adv Gastroenterol. 2025. PMID: 40661219 Free PMC article.
-
Optimum duration of regimens for Helicobacter pylori eradication.Cochrane Database Syst Rev. 2013 Dec 11;2013(12):CD008337. doi: 10.1002/14651858.CD008337.pub2. Cochrane Database Syst Rev. 2013. PMID: 24338763 Free PMC article.
-
Sequential versus standard triple first-line therapy for Helicobacter pylori eradication.Cochrane Database Syst Rev. 2016 Jun 28;2016(6):CD009034. doi: 10.1002/14651858.CD009034.pub2. Cochrane Database Syst Rev. 2016. PMID: 27351542 Free PMC article.
-
Vonoprazan-amoxicillin dual therapy versus bismuth-containing quadruple therapy for Helicobacter pylori eradication: A systematic review and meta-analysis.Helicobacter. 2024 Jan-Feb;29(1):e13040. doi: 10.1111/hel.13040. Epub 2023 Nov 20. Helicobacter. 2024. PMID: 37983865
-
Vonoprazan-based therapies versus PPI-based therapies in patients with H. pylori infection: Systematic review and meta-analyses of randomized controlled trials.Helicobacter. 2024 May-Jun;29(3):e13094. doi: 10.1111/hel.13094. Helicobacter. 2024. PMID: 38790090
References
LinkOut - more resources
Full Text Sources