

Time to Mortality and Predictive Factors Among Adult Heart Failure Patients: Lessons From a Resource-Limited Setting
- PMID: 40821661
- PMCID: PMC12352995
- DOI: 10.1155/crp/3968055
Time to Mortality and Predictive Factors Among Adult Heart Failure Patients: Lessons From a Resource-Limited Setting
Abstract
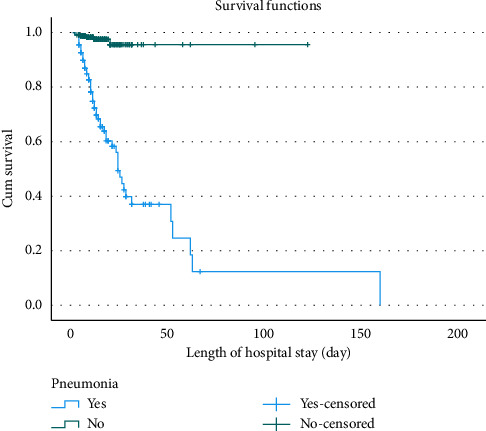
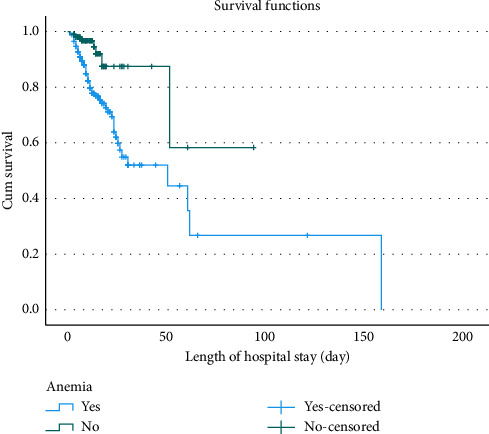
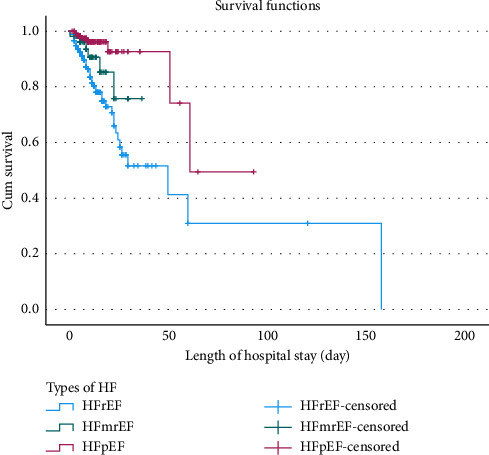
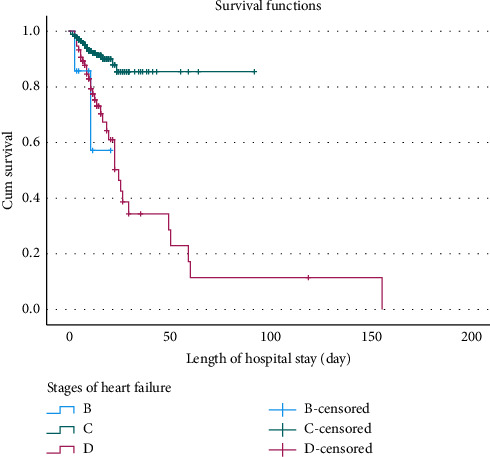
Background: Heart failure (HF) is a major cause of morbidity and mortality in low-resource settings like Ethiopia. This study aimed to assess time to mortality and identify key predictors among adult HF patients at Jimma Medical Center (JMC). Methods: A retrospective cohort study was conducted on 356 adult HF patients admitted to JMC between 2022 and 2023. Survival probabilities were estimated using the Kaplan-Meier method, and Cox proportional hazard regression was used to identify mortality predictors. Results: Among 356 HF patients, 15.7% (95% CI: 12.2%-19.8%) died during the study period. The median hospital stay was 11 days (IQR: 7-17), and the median age was 55 years (IQR: 38-65). Key predictors of higher mortality included hypertension (AHR: 4.6, 95% CI: 1.88-11.61, p < 0.001), pneumonia (AHR: 4.3, 95% CI: 1.15-15.78, p = 0.031), anemia (AHR: 3.3, 95% CI: 1.17-9.06, p = 0.023), acute myocardial infarction (AMI) (AHR: 4.4, 95% CI: 1.9-10.09, p < 0.001), and hyponatremia (AHR: 2.9, 95% CI: 1.44-5.99, p = 0.003). Each unit increase in systolic blood pressure (SBP) and diastolic blood pressure (DBP) was linked to a 7% and 4% lower mortality risk, respectively (p = 0.035). A higher pulse rate was associated with a 4% increased mortality risk. Patients with heart failure with reduced ejection fraction (HFrEF) had a six-fold higher mortality risk compared to those with preserved ejection fraction (HFpEF) (AHR: 6.1, 95% CI: 1.79-24.4, p = 0.008). Conclusion: This study identifies key mortality predictors for HF patients in a resource-limited setting, including hypertension, pneumonia, anemia, AMI, and hyponatremia. The findings emphasize the need for targeted interventions, improved management strategies, and policies to reduce HF mortality in low-resource environments. Further research is needed to refine these findings and enhance care for HF patients in such settings.
Keywords: Cox regression; Ethiopia; Kaplan–Meier estimator; heart failure; mortality.
Copyright © 2025 Elsah Tegene Asefa et al. Cardiology Research and Practice published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Time to death and its predictors among women with uterine rupture admitted to jimma town public hospitals, South West Ethiopia: retrospective cohort study.BMC Pregnancy Childbirth. 2025 Jul 2;25(1):703. doi: 10.1186/s12884-025-07817-4. BMC Pregnancy Childbirth. 2025. PMID: 40604663 Free PMC article.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Exercise-based rehabilitation for heart failure.Cochrane Database Syst Rev. 2014 Apr 27;2014(4):CD003331. doi: 10.1002/14651858.CD003331.pub4. Cochrane Database Syst Rev. 2014. Update in: Cochrane Database Syst Rev. 2019 Jan 29;1:CD003331. doi: 10.1002/14651858.CD003331.pub5. PMID: 24771460 Free PMC article. Updated.
-
Survival status and predictors of mortality among adult Stroke patients admitted to Jimma University Medical Center, South west Ethiopia: A retrospective Cohort study.Vasc Health Risk Manag. 2023 Aug 25;19:527-541. doi: 10.2147/VHRM.S399815. eCollection 2023. Vasc Health Risk Manag. 2023. PMID: 37649671 Free PMC article.
-
Dietary Approaches to Stop Hypertension (DASH) for the primary and secondary prevention of cardiovascular diseases.Cochrane Database Syst Rev. 2025 May 6;5(5):CD013729. doi: 10.1002/14651858.CD013729.pub2. Cochrane Database Syst Rev. 2025. PMID: 40326569 Review.
References
-
- Heidenreich P. A., Bozkurt B., Aguilar D., et al. 2022 aha/acc/hfsa Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Journal of the American College of Cardiology . 2022;79(17):e263–e421. doi: 10.1016/j.jacc.2021.12.012. - DOI - PubMed
-
- Moyehodie Y. A., Muluneh M. W., Belay A. T., Fenta S. M. Time to Death and Its Determinant Factors Among Patients With Chronic Heart Failure in Northwest Ethiopia: A Retrospective Study at Selected Referral Hospitals. Frontiers in Cardiovascular Medicine . 2022;9 doi: 10.3389/fcvm.2022.817074. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
