

Case Report: Eculizumab in highly active myasthenia gravis complicated by severe infections
- PMID: 40821799
- PMCID: PMC12350286
- DOI: 10.3389/fimmu.2025.1596283
Case Report: Eculizumab in highly active myasthenia gravis complicated by severe infections
Abstract
Highly active myasthenia gravis refers to a subset of refractory patients who exhibit recurrent exacerbations and crises. Eculizumab, a complement C5 inhibitor, has shown its efficacy and safety for patients with anti-acetylcholine receptor antibody-positive(AchR +)refractory generalized myasthenia gravis(gMG) in the REGAIN trial. However, the efficacy and safety of eculizumab in treating MG patients with severe infections have not yet been supported by clinical evidence. This is a case series reporting four patients with highly active myasthenia gravis complicated by severe infections. Changes in Myasthenia Gravis-Activities of Daily Living (MG-ADL) and Quantitative Myasthenia Gravis (QMG) scores were recorded before and after 12 injections of eculizumab to assess efficacy. Pathogen characteristics of infections were summarized using bacterial culture and next-generation sequencing (NGS) results, presented as a heatmap to illustrate pathogen species and abundance. Inflammatory markers, including Procalcitonin (PCT), C-Reactive Protein (CRP), neutrophil count, and total lymphocyte count, were monitored to evaluate the safety. Treatment regimens were retrospectively analyzed to further assess clinical outcomes and safety. The baseline ADL data for the four patients was 22 ± 2.31 (Mean ± SD), and the baseline QMG data was 30.5 ± 8.23. After 12 injections of eculizumab treatment, the scores decreased to ADL 4.75 ± 3.3 and QMG 14 ± 3.37. During the treatment, no apparent worsening of infections related to Eculizumab was noted. Three patients successfully had their tracheostomy tubes removed, and none of the four patients experienced further myasthenic crises. Eculizumab demonstrated clinical improvement in this series, and the treatment was well-tolerated. This case series addresses the need for data on complement inhibitors in highly active myasthenia gravis patients with severe infections, provides clinical reference support for the expanded application of eculizumab.
Keywords: case series; complement inhibition; eculizumab; highly active myasthenia gravis; severe infections.
Copyright © 2025 Deng, Luo, Zhang, Yang, Wang, Zhang, Yan, Yang and Jiang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



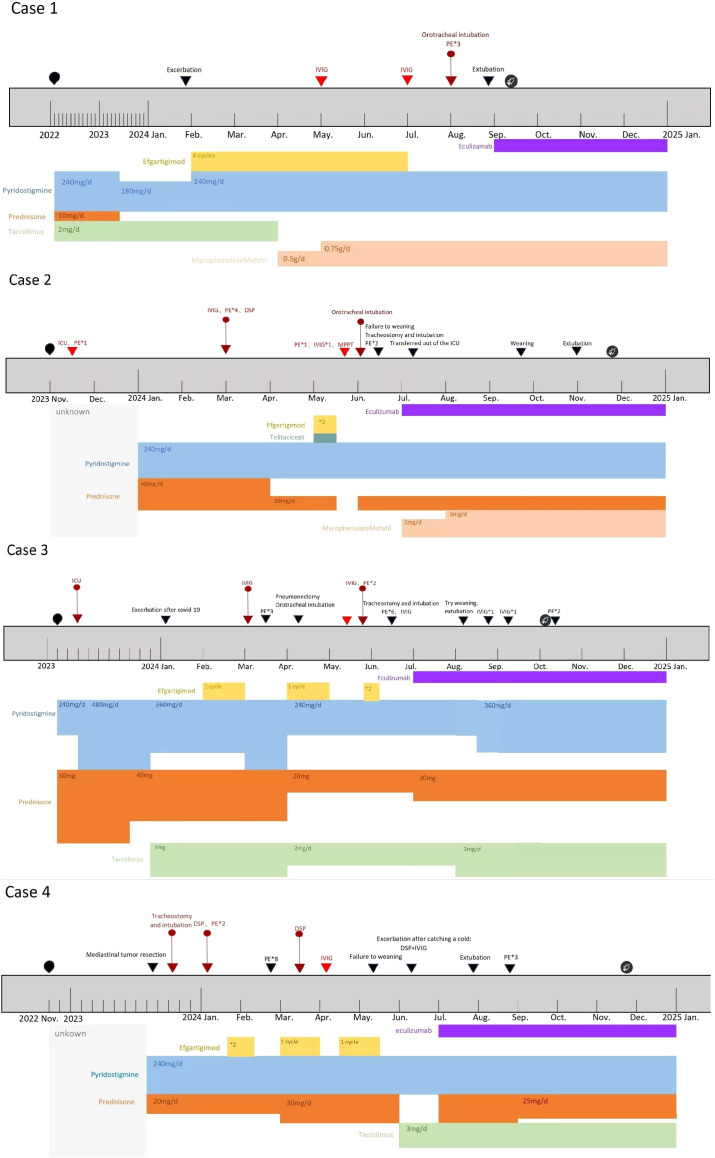
 : Time points of meningococcal vaccination in four Patients. The type of vaccine administered: ACYW135 meningococcal polysaccharide vaccine.
: Time points of meningococcal vaccination in four Patients. The type of vaccine administered: ACYW135 meningococcal polysaccharide vaccine.  :Onset time of the disease. ▼: Timing of disease progression and significant treatment.
:Onset time of the disease. ▼: Timing of disease progression and significant treatment.  :Myasthenic Crisis (MC).
:Myasthenic Crisis (MC).  :Impending Myasthenia crisis (IMC). DSP, Dexamethasone sodium phosphate pulse therapy. MPPT, Methylprednisolone pulse therapy. Efgartigimod administration: 1 cycle = 4 injections, once per week. The injection dose is calculated based on the patient’s body weight by 10 mg/kg. Unknown:For Case 2, the initial treatment details are unclear due to delayed diagnosis. For Case 4, the initial treatment details are unclear due to incomplete patient recall.
:Impending Myasthenia crisis (IMC). DSP, Dexamethasone sodium phosphate pulse therapy. MPPT, Methylprednisolone pulse therapy. Efgartigimod administration: 1 cycle = 4 injections, once per week. The injection dose is calculated based on the patient’s body weight by 10 mg/kg. Unknown:For Case 2, the initial treatment details are unclear due to delayed diagnosis. For Case 4, the initial treatment details are unclear due to incomplete patient recall.Similar articles
-
Switching to subcutaneous zilucoplan from intravenous complement component 5 inhibitors in generalised myasthenia gravis: a phase IIIb, open-label study.Ther Adv Neurol Disord. 2025 Jul 5;18:17562864251347283. doi: 10.1177/17562864251347283. eCollection 2025. Ther Adv Neurol Disord. 2025. PMID: 40620733 Free PMC article.
-
First analysis of the Myasthenia Gravis SPOTLIGHT Registry: outcomes with eculizumab and ravulizumab.J Neurol Sci. 2025 Sep 15;476:123628. doi: 10.1016/j.jns.2025.123628. Epub 2025 Jul 16. J Neurol Sci. 2025. PMID: 40812271
-
Risk-Benefit Analysis of Novel Treatments for Patients with Generalized Myasthenia Gravis.Adv Ther. 2024 Dec;41(12):4628-4647. doi: 10.1007/s12325-024-03014-5. Epub 2024 Oct 29. Adv Ther. 2024. PMID: 39470879 Free PMC article.
-
Clinical Efficacy and Safety of Eculizumab for Treating Myasthenia Gravis.Front Immunol. 2021 Aug 11;12:715036. doi: 10.3389/fimmu.2021.715036. eCollection 2021. Front Immunol. 2021. PMID: 34456922 Free PMC article.
-
Rituximab for myasthenia gravis.Cochrane Database Syst Rev. 2025 Jul 3;7(7):CD014574. doi: 10.1002/14651858.CD014574.pub2. Cochrane Database Syst Rev. 2025. PMID: 40607605 Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous