

A mechanistic computational model of HGF-VEGF-mediated endothelial cell proliferation and vascular permeability
- PMID: 40822341
- PMCID: PMC12355113
- DOI: 10.1016/j.isci.2025.113199
A mechanistic computational model of HGF-VEGF-mediated endothelial cell proliferation and vascular permeability
Abstract
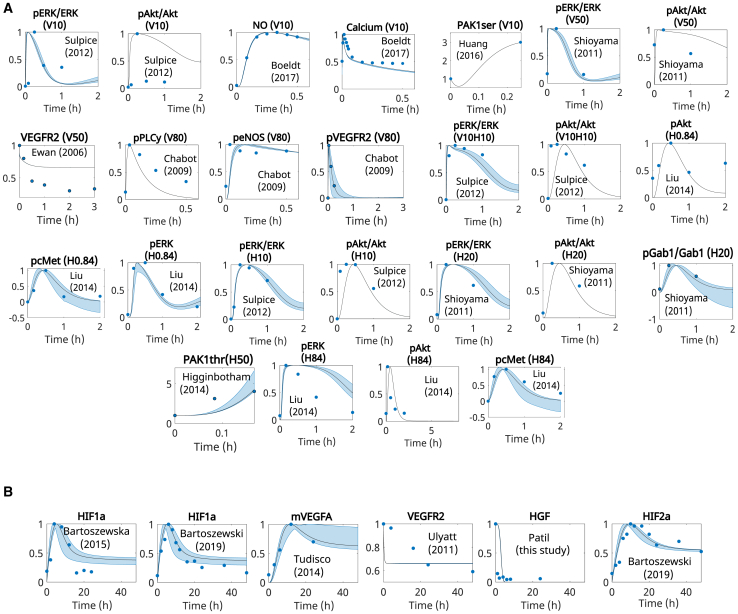
Hepatocyte growth factor (HGF) and vascular endothelial growth factor (VEGF) are important pro-angiogenic factors in angiogenesis-dependent diseases. While sharing some signaling pathways, their contrasting effect on vascular permeability remains under investigation. To explore how these factors promote angiogenesis, we developed, calibrated, and validated a data-driven mechanistic computational model of HGF and VEGF signaling in endothelial cells (ECs). We proposed that variations in permeability profiles may stem from RAC1-PAK1 activation via site-specific phosphorylation. By introducing permeability and proliferation indices, our simulations indicated a dose-dependent effect of VEGF that hampered the ability of HGF to promote vascular stability. Our simulations indicate that HGF did not require VEGFR2 activation to affect permeability and proliferation. This model has the potential to be applicable and helpful in analyzing angiogenesis-dependent diseases. It provided insights into the mechanisms of EC proliferation and vascular permeability induced by HGF and VEGF and permitted evaluation of their separate or combined effects.
Keywords: Biological constraints; Experimental models in systems biology; In silico biology; Integrative aspects of cell biology.
© 2025 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures








Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Impact of ligand binding on VEGFR1, VEGFR2, and NRP1 localization in human endothelial cells.PLoS Comput Biol. 2025 Jul 16;21(7):e1013254. doi: 10.1371/journal.pcbi.1013254. eCollection 2025 Jul. PLoS Comput Biol. 2025. PMID: 40668864 Free PMC article.
-
Anti-vascular endothelial growth factor biosimilars for neovascular age-related macular degeneration.Cochrane Database Syst Rev. 2024 Jun 3;6(6):CD015804. doi: 10.1002/14651858.CD015804.pub2. Cochrane Database Syst Rev. 2024. PMID: 38829176 Free PMC article.
-
MAPK Signaling and Angiopoietin-2 Contribute to Endothelial Permeability in Capillary Malformations.bioRxiv [Preprint]. 2025 Apr 5:2025.03.31.646063. doi: 10.1101/2025.03.31.646063. bioRxiv. 2025. PMID: 40235979 Free PMC article. Preprint.
-
Factors that influence parents' and informal caregivers' views and practices regarding routine childhood vaccination: a qualitative evidence synthesis.Cochrane Database Syst Rev. 2021 Oct 27;10(10):CD013265. doi: 10.1002/14651858.CD013265.pub2. Cochrane Database Syst Rev. 2021. PMID: 34706066 Free PMC article.
References
-
- Teo Z.L., Tham Y.-C., Yu M., Chee M.L., Rim T.H., Cheung N., Bikbov M.M., Wang Y.X., Tang Y., Lu Y., et al. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045: Systematic Review and Meta-analysis. Ophthalmology. 2021;128:1580–1591. doi: 10.1016/j.ophtha.2021.04.027. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
