

Association between serum anion gap trajectory and mortality in hospitalized patients with sepsis: an analysis of the MIMIC-IV database
- PMID: 40822945
- PMCID: PMC12353743
- DOI: 10.3389/fendo.2025.1578078
Association between serum anion gap trajectory and mortality in hospitalized patients with sepsis: an analysis of the MIMIC-IV database
Abstract
Background: Sepsis remains a leading cause of mortality in intensive care units (ICUs), with high morbidity and healthcare costs worldwide. The serum anion gap (AG), a marker of metabolic acidosis, has been associated with adverse outcomes in various critical illnesses. However, the prognostic value of longitudinal AG trajectories in sepsis remains underexplored. This study explored the link between dynamic AG trajectories and all-cause mortality in critically ill septic patients.
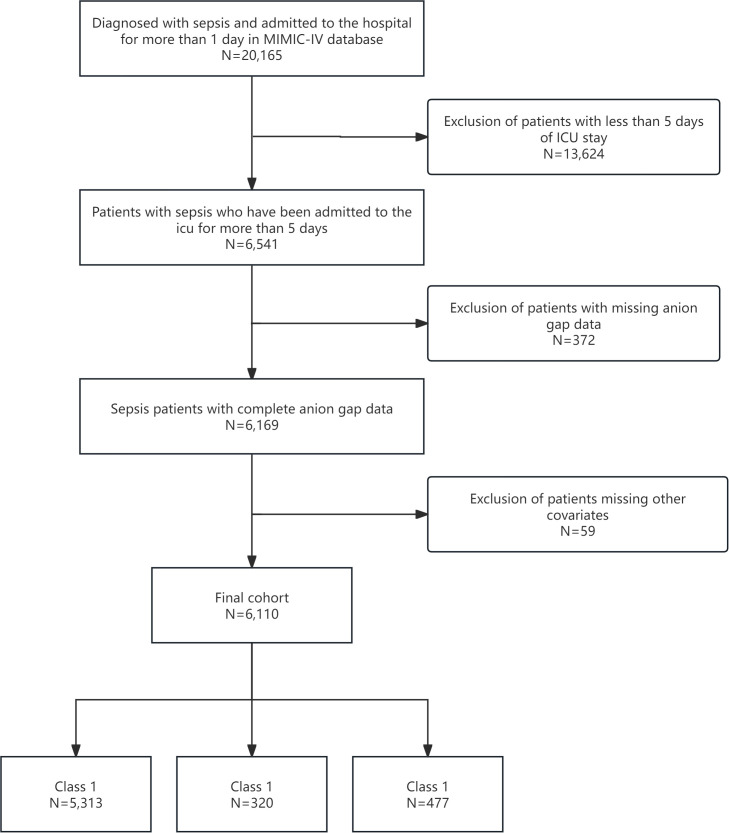
Methods: A retrospective cohort study utilized data from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database. Adult patients meeting Sepsis-3 criteria for sepsis were included. Group-based trajectory modeling was used to identify AG trajectories during the initial five days of ICU admission. Patients were classified into three trajectory groups: normal-level-stable trajectory (Class 1), high-level-decline trajectory (Class 2), and progressive acidosis trajectory (Class 3). Cox proportional hazards models evaluated the link between AG trajectories and ICU/hospital mortality, controlling for demographic, laboratory, and clinical severity factors. Subgroup and sensitivity analyses were performed to validate the findings.
Results: Among 6,110 septic patients, three distinct AG trajectory groups were identified. Patients in Class 3 (decreasing high AG) had the highest mortality, with ICU mortality of 30.61% and hospital mortality of 35.85%, compared to Class 1 (ICU mortality: 14.46%, hospital mortality: 19.41%) and Class 2 (ICU mortality: 21.88%, hospital mortality: 31.88%). In fully adjusted models, Class 3 exhibited a significantly increased risk of ICU mortality [HR=1.72, (95% CI 1.43-2.07), P<0.001] and hospital mortality [HR=1.64, (95% CI 1.39-1.94), P<0.001] relative to Class 1. Subgroup analysis revealed a significant interaction between AG trajectories and heart failure status. Sensitivity analysis excluding patients with malignancies confirmed the robustness of the findings.
Conclusion: Continuous monitoring of AG levels is crucial for risk assessment and personalized treatment, as rising AG levels significantly increase mortality risk. These findings underscore the potential of AG trajectories as a dynamic biomarker to improve sepsis management and patient outcomes.
Keywords: anion gap; intensive care unit; mortality; sepsis; trajectory analysis.
Copyright © 2025 Jing, Shi, Xu, Zhao, Li and Qin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Markwart R, Saito H, Harder T, Tomczyk S, Cassini A, Fleischmann-Struzek C, et al. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. (2020) 46:1536–51. doi: 10.1007/s00134-020-06106-2, PMID: - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous