

EBV-positive inflammatory follicular dendritic cell sarcoma occurring in different organs: a case report and literature review
- PMID: 40823092
- PMCID: PMC12351499
- DOI: 10.3389/fonc.2025.1603496
EBV-positive inflammatory follicular dendritic cell sarcoma occurring in different organs: a case report and literature review
Abstract
Background: Epstein-Barr virus (EBV)-positive inflammatory follicular dendritic cell sarcoma (EBV+ IFDCS) represents a low-grade malignancy arising from the proliferation of follicular dendritic cells. This distinct and rare subtype, characterized by abundant lymphoplasmacytic infiltration, is closely linked to EBV infection and is seldom encountered in clinical practice.
Methods: Presented here are three cases of primary EBV+ IFDCS, occurring in the liver and spleen. This study systematically analyzed the clinical presentations, radiological features, and pathological characteristics of our cases. Additionally, we conducted a comprehensive review of the respective characteristics documented in the existing literature.
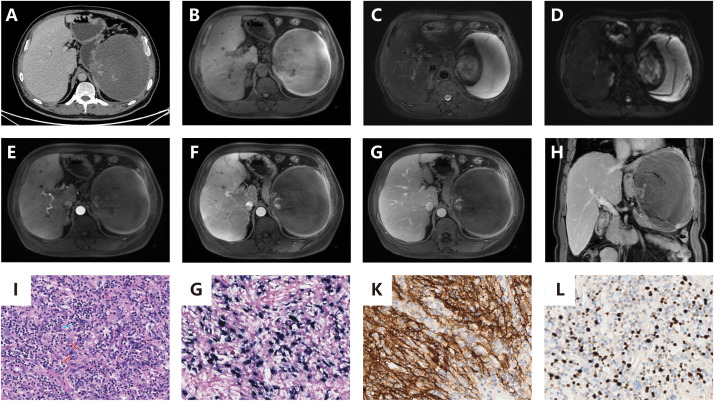
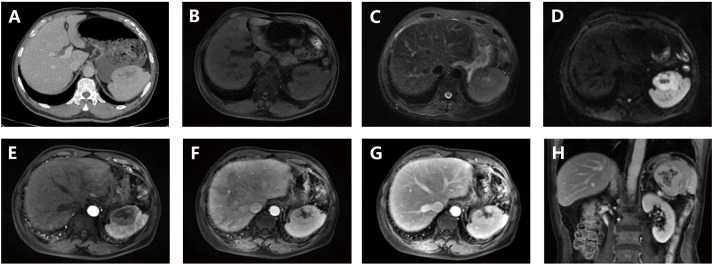
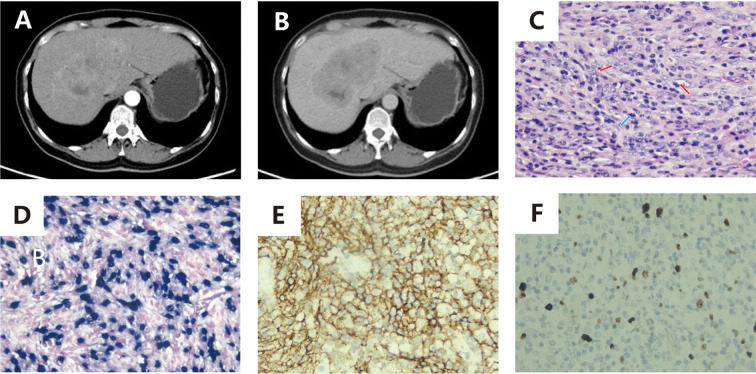
Results: We present three cases of EBV+ IFDCS, with lesions localized to the spleen (n=2) and liver (n=1). Notably, only one patient developed clinical symptoms secondary to splenic mass rupture and post-embolization sequelae, while the remaining cases were identified incidentally without associated symptomatology. All three patients underwent preoperative contrast-enhanced magnetic resonance imaging (CT) scans demonstrating solitary, well-circumscribed round masses/nodules. The two splenic lesions exhibited necrotic-cystic degeneration and one displayed a capsule, with absence of calcification in all cases. Tumor parenchyma showed mild arterial-phase enhancement and partial delayed-phase washout. The two splenic cases underwent additional magnetic resonance imaging (MRI) evaluation, revealing restricted diffusion in the solid tumor components and apparent diffusion coefficient (ADC) values comparable to the surrounding splenic parenchyma. Complete surgical excision was performed in all patients, and histopathological evaluation confirmed the diagnosis of EBV+ IFDCS through immunohistochemical analysis. As of the latest follow-up, all three patients are alive.
Conclusion: EBV+ IFDCS is a rare condition that primarily arises in the liver and spleen, with prognosis varying among patients with primary tumors in different organs. This study presents three cases of EBV+ IFDCS that occurred in diverse anatomical locations, examines their clinical, radiological, pathological features and differential diagnoses, and aims to deepen the understanding of clinicians and radiologists regarding this form of Mesenchymal dendritic cell neoplasm.
Keywords: EBV-positive inflammatory follicular dendritic cell sarcoma; Epstein-Barr virus; case report; computed tomography; magnetic resonance imaging.
Copyright © 2025 Bai, Hu and Zhu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Lennert K. Malignant lymphomas other than hodgkin’s disease. Berlin, Heidelberg: Springer; (1978) p. 51–68.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials