

Prevalence of locoregional and distant lymph node metastases in children and adolescents/young adults with soft tissue sarcomas: a Bayesian meta-analysis of proportions
- PMID: 40823497
- PMCID: PMC12355419
- DOI: 10.1016/j.eclinm.2025.103390
Prevalence of locoregional and distant lymph node metastases in children and adolescents/young adults with soft tissue sarcomas: a Bayesian meta-analysis of proportions
Abstract
Background: The presence of both regional and distant lymph node metastases (LNM) in paediatric and adolescent/young adult (AYA) patients with soft tissue sarcomas (STS) significantly impacts clinical outcomes. However, reported rates of LNM vary widely across the literature and are often accompanied by substantial uncertainty. We aimed to quantitatively synthesise global proportions of LNM across different histological subtypes and tumour sites in this population.
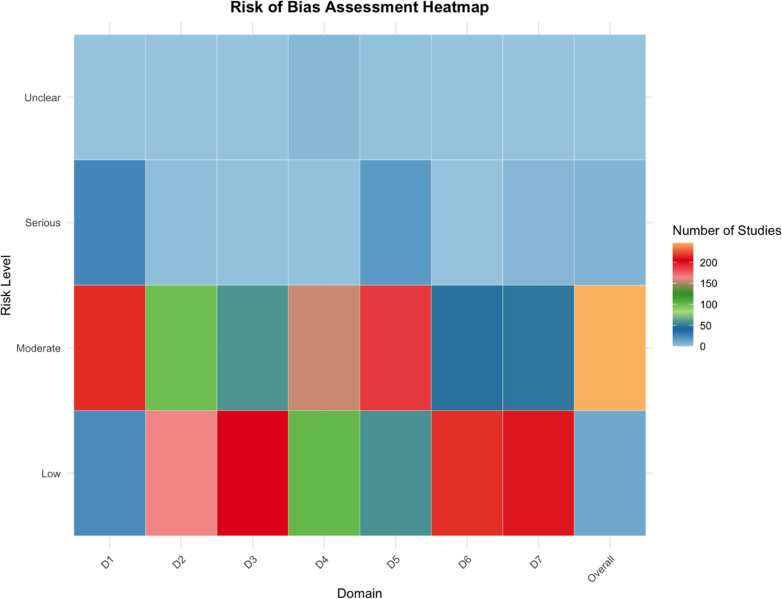
Methods: In this meta-analysis, we systematically searched MEDLINE, Scopus, and Web of Science from inception until May 1, 2024 (updated on June 1, 2025) for studies published in English that reported LNM rates in patients with STS aged 0-21 years. Eligible study designs included cohort studies, case-control studies, case series, and randomised controlled trials. Patient-level data were not requested from study authors. LNM had to be confirmed clinically, by imaging, or histologically. We excluded reviews, editorials, and case reports with fewer than three patients. We conducted a random-effects Bayesian meta-analysis using a logit transformation to synthesise LNM proportions. The posterior distributions of LNM prevalence were summarised by the posterior mean and 95% credible intervals (CrIs). Study quality was assessed across seven domains: confounding, participant selection, exposure classification, deviations from intended exposures, missing data, outcome measurement, and selective reporting.
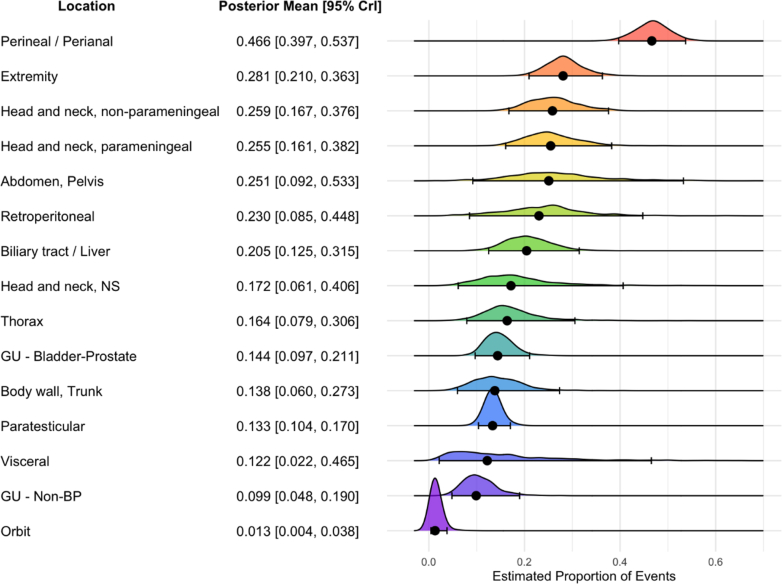
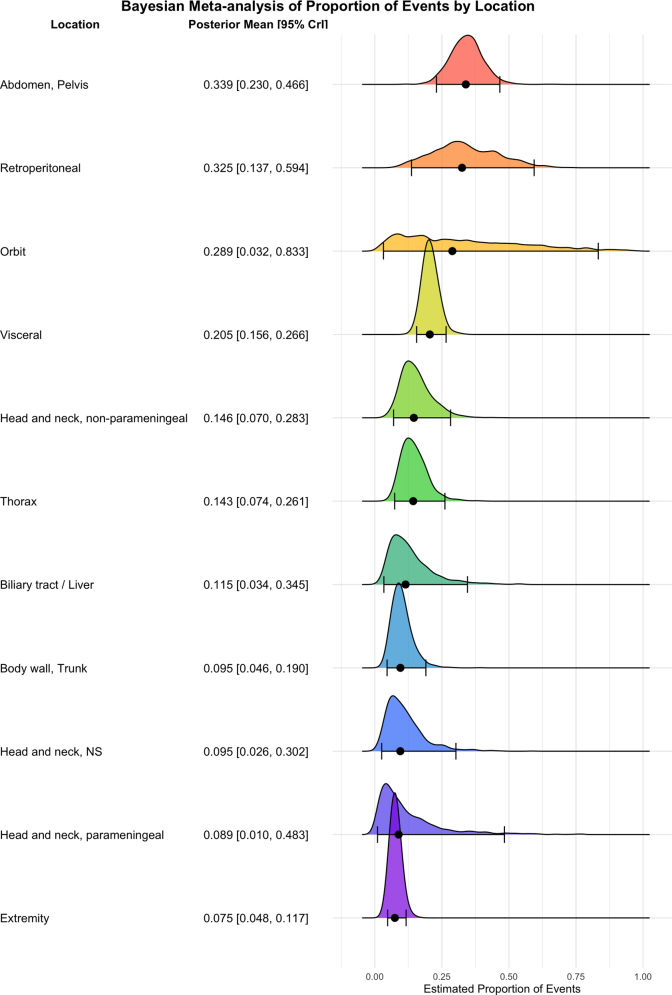
Findings: Of 3969 records screened, 263 articles were included in the data synthesis. These comprised 147 studies on rhabdomyosarcoma (RMS), 106 on non-rhabdomyosarcoma soft tissue sarcoma (NRSTS), and 10 on mixed RMS/NRSTS cohorts, representing 53,093 patients with STS. The pooled posterior mean proportion of LNM in patients with RMS (n = 41,547) was 0.228 (95% CrI: 0.202-0.255), with the highest rates observed in patients with alveolar RMS (posterior mean proportion: 0.370; 95% CrI: 0.276-0.473). Subgroup analysis by RMS primary site revealed the highest LNM rates in the perianal/perineal region (0.466; 95% CrI: 0.397-0.537), extremity (0.281; 0.210-0.363), and non-parameningeal head/neck region (0.259; 0.167-0.376). Among patients with NRSTS (n = 11,546), the pooled posterior mean proportion of LNM was 0.111 (95% CrI: 0.092-0.133), with desmoplastic small round cell tumour (0.440; 0.335-0.552), clear cell sarcoma (0.212; 0.163-0.275), and malignant rhabdoid tumour (0.199; 0.141-0.273) showing the highest rates. Most analyses had moderate-to-high heterogeneity (95% CrI for tau: 0.7443-1.1139).
Interpretation: Our Bayesian meta-analysis synthesises global evidence on the prevalence of LNM in paediatric and AYA patients with STS, highlighting the significant heterogeneity in LNM rates by histological subtype, particularly in NRSTS, and by tumour location, especially in RMS. Future studies should aim to standardise lymph node staging protocols and reporting practices to improve classification accuracy and enhance comparability across studies.
Funding: None.
Keywords: Bayesian meta-analysis; Lymph node metastases; Rhabdomyosarcoma; Soft tissue sarcomas; ‘Non-rhabdomyosarcoma’ soft tissue sarcoma.
© 2025 The Author(s).
Conflict of interest statement
We declare no competing interests.
Figures



Similar articles
-
Autologous hematopoietic stem cell transplantation following high dose chemotherapy for non-rhabdomyosarcoma soft tissue sarcomas.Cochrane Database Syst Rev. 2013 Aug 7;2013(8):CD008216. doi: 10.1002/14651858.CD008216.pub4. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2017 Apr 13;4:CD008216. doi: 10.1002/14651858.CD008216.pub5. PMID: 23925699 Free PMC article. Updated.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2020 Jan 9;1(1):CD011535. doi: 10.1002/14651858.CD011535.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Apr 19;4:CD011535. doi: 10.1002/14651858.CD011535.pub4. PMID: 31917873 Free PMC article. Updated.
-
Systemic treatments for metastatic cutaneous melanoma.Cochrane Database Syst Rev. 2018 Feb 6;2(2):CD011123. doi: 10.1002/14651858.CD011123.pub2. Cochrane Database Syst Rev. 2018. PMID: 29405038 Free PMC article.
References
LinkOut - more resources
Full Text Sources
