

Improvement in functional and mental outcomes after resection rectopexy for obstructive defecation syndrome ODS
- PMID: 40825813
- PMCID: PMC12361406
- DOI: 10.1038/s41598-025-15037-1
Improvement in functional and mental outcomes after resection rectopexy for obstructive defecation syndrome ODS
Abstract
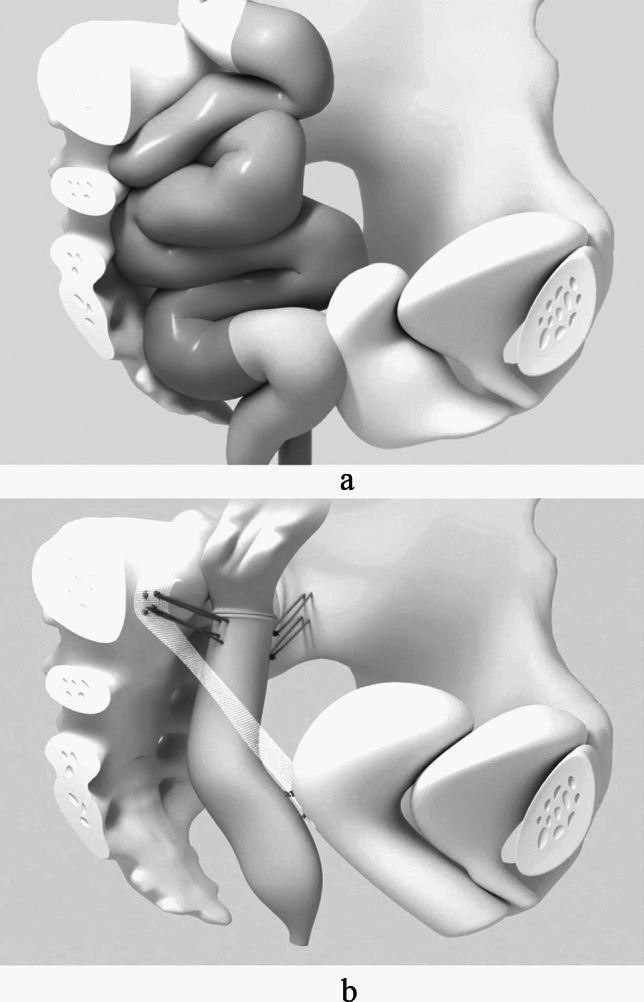
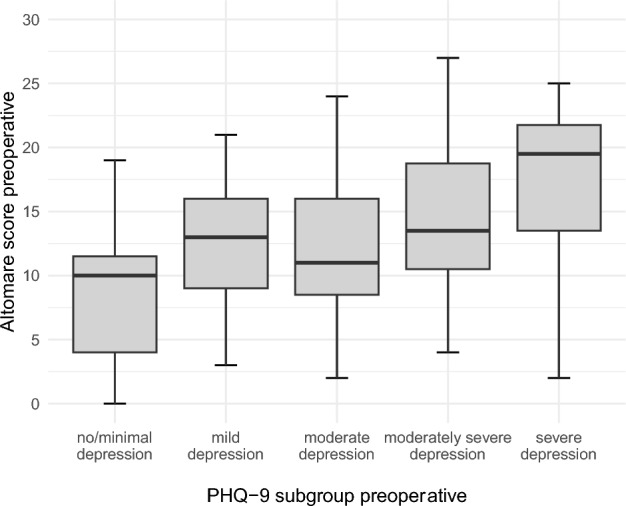
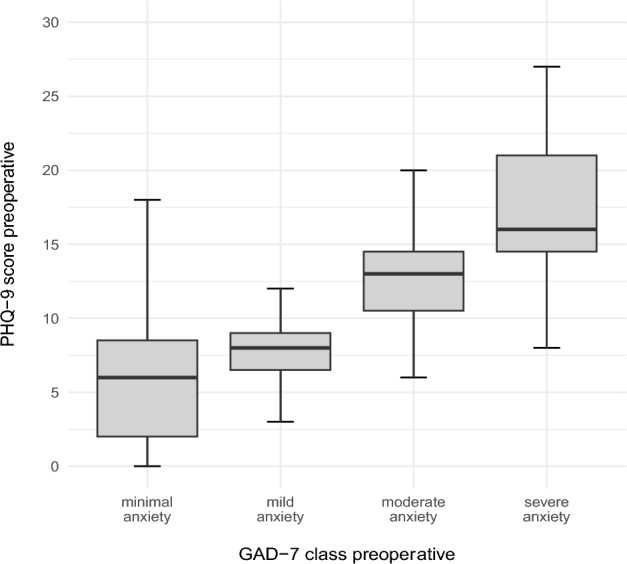
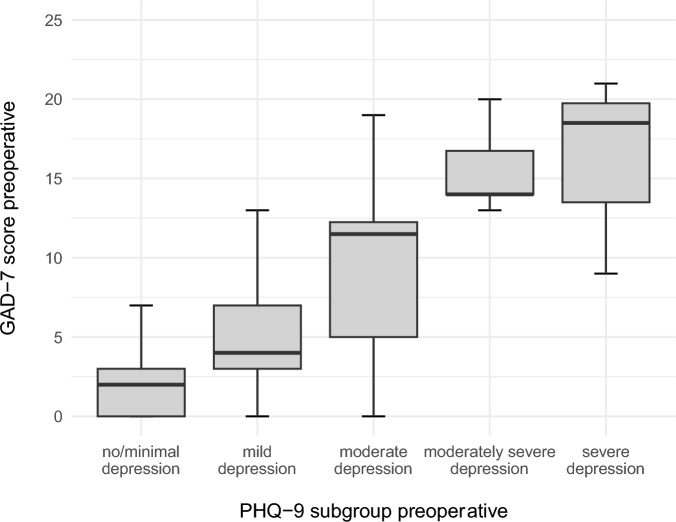
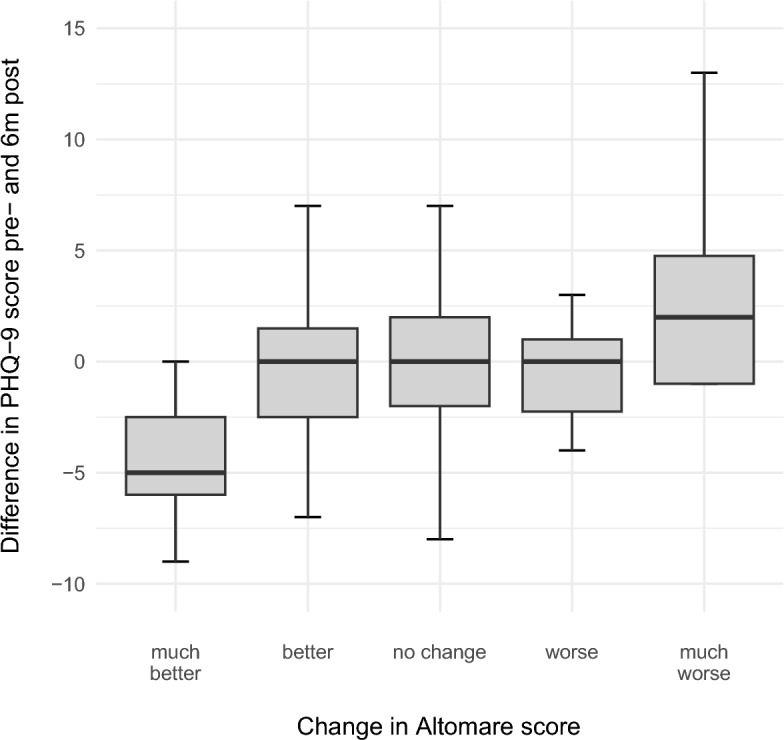
Obstructive defecation syndrome (ODS) is a condition that causes straining and may require manual evacuation and patients' thoughts circle around defecation impairing their quality of life. Mental comorbidity-related findings suggest a mental burden in ODS patients. In an observational cohort design, this study investigated the relationship between the mental distress and their clinical symptom severity for a group of patients with ODS who underwent surgical treatment. This study included 108 consecutive patients with ODS who were scheduled for laparoscopic resection rectopexy combined with pelvic floor repair, if indicated. Clinical symptom severity (Altomare score, rectal toxicity score, and Wexner incontinence score) and mental health scores (Generalized Anxiety Disorder-7 [GAD-7] and Personal Health Questionnaire-9 [PHQ-9]) were assessed before and 6 months after surgery. Before surgery, 82.5% of patients had at least mild depressive symptoms (PHQ-9 score ≥ 5), and 55.6% of patients had at least mild anxiety (GAD-7 score ≥ 5). The severity of the mental health scores correlated with the clinical symptom severity. At the 6-month follow-up, the bowel function scores improved significantly. Depression symptoms improved, whereas only slight changes in anxiety symptoms were observed. The improvement in clinical symptom severity correlated with better mental score results, whereas the severity of the preoperative mental distress did not influence the surgical or follow-up outcomes. Patients with obstructive defecation syndrome (ODS) experience significant depression and anxiety that adversely affect their quality of life. Surgical improvement of bowel function reduces depressive symptoms and, to a lesser extent, anxiety symptoms. Early multidisciplinary intervention should be considered for effective management. Future studies should further investigate mental distress caused by ODS symptoms or other underlying psychiatric comorbidities.
Keywords: Anxiety; Depression; Interdisciplinary surgery; Mental burden; Mental outcome; Obstructed defecation syndrome (ODS).
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: Sebastian Ludwig receives honoraria for speaking at symposia from the FEG Textiltechnik GmbH Aachen, Germany. All other authors have no financial or non-financial interests that are directly or indirectly related to the work submitted for publication and have no competing interests to report. Ethics approval: This retrospective chart review study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. No animals were included in this research study. The study was approved by the Ethic Committee of the Aerztekammer Northrhine in Duesseldorf, Germany (No. 74/2024). Informed consent: All patients involved in the study gave their written informed consent. All humans involved gave their written informed consent. No animals were included in this research study.
Figures






Similar articles
-
Imaging modalities for the detection of posterior pelvic floor disorders in women with obstructed defaecation syndrome.Cochrane Database Syst Rev. 2021 Sep 23;9(9):CD011482. doi: 10.1002/14651858.CD011482.pub2. Cochrane Database Syst Rev. 2021. PMID: 34553773 Free PMC article.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Long-Term Outcomes of Transvaginal Sacrospinous Ligament Suture Rectopexy.Int Urogynecol J. 2025 Jul;36(7):1425-1433. doi: 10.1007/s00192-025-06099-w. Epub 2025 Mar 5. Int Urogynecol J. 2025. PMID: 40042604
-
[Guidelines for the prevention and management of bronchial asthma (2024 edition)].Zhonghua Jie He He Hu Xi Za Zhi. 2025 Mar 12;48(3):208-248. doi: 10.3760/cma.j.cn112147-20241013-00601. Zhonghua Jie He He Hu Xi Za Zhi. 2025. PMID: 40050074 Chinese.
-
Tonsillectomy or adenotonsillectomy versus non-surgical management for obstructive sleep-disordered breathing in children.Cochrane Database Syst Rev. 2015 Oct 14;2015(10):CD011165. doi: 10.1002/14651858.CD011165.pub2. Cochrane Database Syst Rev. 2015. PMID: 26465274 Free PMC article.
References
-
- Lukies, M., Harisis, G., Jarema, A., Scicchitano, M. & MacLaurin, W. Defecating proctography: A pictorial essay. Radiography28, 628–633. 10.1016/j.radi.2022.04.012 (2022). - PubMed
-
- Saunders, W. B. Constipation. In Surgery of the Anus, Rectum & Colon 3rd edn (eds Keighley, M. R. B. et al.) 693–740 (Elsevier, 2008).
-
- Andromanakos, N., Skandalakis, P., Troupis, T. & Filippou, D. Constipation of anorectal outlet obstruction: pathophysiology, evaluation and management. J. Gastroenterol. Hepatol.10.1111/j.1440-1746.2006.04333.x (2006). - PubMed
-
- Hedrick, T. L. & Friel, C. M. Constipation and pelvic outlet obstruction. Gastroenterol. Clin. North Am.42, 863–876. 10.1016/j.gtc.2013.09.004 (2013). - PubMed
LinkOut - more resources
Full Text Sources
