

Diagnostic value of the urea-to-creatinine ratio for gastrointestinal bleeding source: influence of renal function
- PMID: 40826036
- PMCID: PMC12359887
- DOI: 10.1186/s12882-025-04382-y
Diagnostic value of the urea-to-creatinine ratio for gastrointestinal bleeding source: influence of renal function
Abstract
Background: Gastrointestinal (GI) bleeding is frequent and clinically critical, especially in patients with renal dysfunction. Localization of the source is relevant for treatment and outcomes. The urea-to-creatinine ratio (UCR) has been proposed as a tool to differentiate between upper and lower GI bleeding. However, its diagnostic utility across varying degrees of renal impairment remains unclear.
Methods: From January 2021 to October 2023, all patients with suspected GI bleeding who underwent endoscopy were retrospectively analyzed in a single center. Patients without confirmed bleeding were excluded. Patients were stratified by renal function: normal renal function, chronic kidney disease (CKD), acute kidney injury (AKI), and AKI with pre-existing CKD (acute-on-chronic). We assessed the discriminatory power of the UCR to distinguish upper from lower GI bleeding within each group.
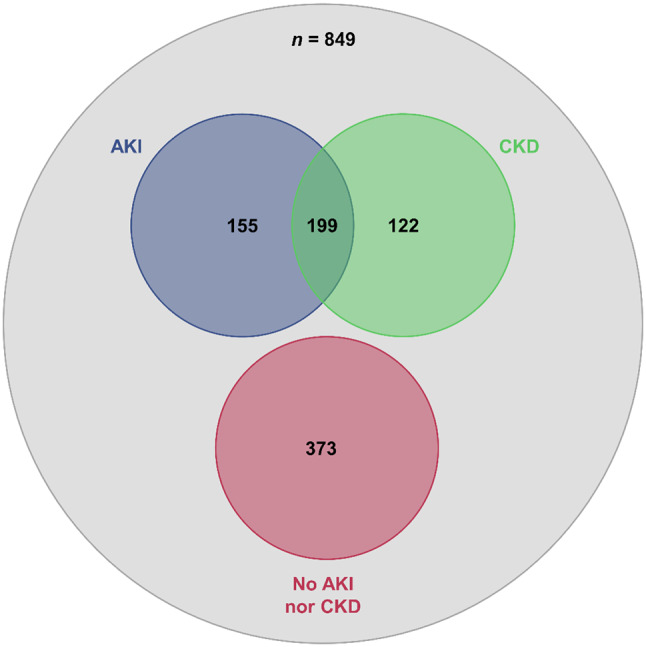
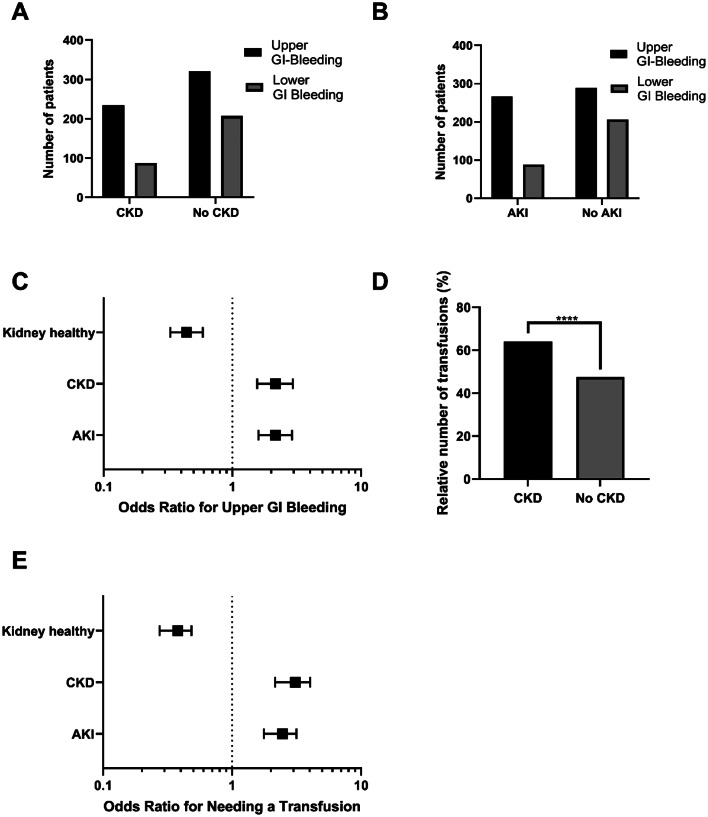
Results: A total of 849 patients (mean age 66.9 ± 18.2 years) were included. Approximately two-thirds of the patients (n = 544; 64.1%) were male. CKD was present in 321 (37.8%) and AKI in 354 (41.7%) patients; 199 (56.2%) of those with AKI had pre-existing CKD. Upper GI bleeding occurred more frequently in patients with AKI (75.1%) and CKD (72.9%) than in those with normal renal function (p < 0.0001 and p = 0.0003, respectively); both groups also required transfusions more frequently (p < 0.0001 for both). UCR values were significantly higher in upper vs. lower GI bleeding in patients with normal renal function (67.5 vs. 42.5; p < 0.0001), but this difference was reduced in CKD (49.3 vs. 41.0; p = 0.0103) and not significant in AKI (53.1 vs. 47.7; p = 0.09). The diagnostic performance of UCR was best in patients with normal renal function (AUROC 0.69) and markedly impaired in CKD (AUROC 0.56) and AKI (AUROC 0.54).
Conclusion: The diagnostic value of UCR to localize GI bleeding depends strongly on renal function. While the UCR may help to identify the bleeding site in patients with normal kidney function, impaired renal function hampers the reliability of the UCR, especially in patients with AKI. As renal dysfunction is common in patients with GI bleeding, kidney function must be taken into account when interpreting UCR values.
Supplementary Information: The online version contains supplementary material available at 10.1186/s12882-025-04382-y.
Keywords: Acute kidney injury (AKI); Chronic kidney disease (CKD); Endoscopy; Gastrointestinal (GI) bleeding; Renal dysfunction; Urea-to-creatinine ratio (UCR).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Ethics Committee of the Faculty of Medicine at the University of Marburg (File Number “23–41 RS”). As the study was conducted retrospectively and involved only the collection of routine clinical parameters, which were analyzed in anonymized form, no identification of individual participants was possible. In accordance with the applicable regulations, explicit informed consent from the patients was not required. This research was carried out in accordance with the Declaration of Helsinki of the World Medical Association and complied with local guidelines for human studies. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Kamboj AK, Hoversten P, Leggett CL. Upper gastrointestinal bleeding: etiologies and management. Mayo Clinic Proceedings. 2019;94:697–703. 10.1016/j.mayocp.2019.01.022 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
