

Subtraction fractional flow reserve with computed tomography and pericoronary fat attenuation index enhances the identification of revascularization needs in patients
- PMID: 40826046
- PMCID: PMC12362918
- DOI: 10.1186/s12880-025-01874-z
Subtraction fractional flow reserve with computed tomography and pericoronary fat attenuation index enhances the identification of revascularization needs in patients
Abstract
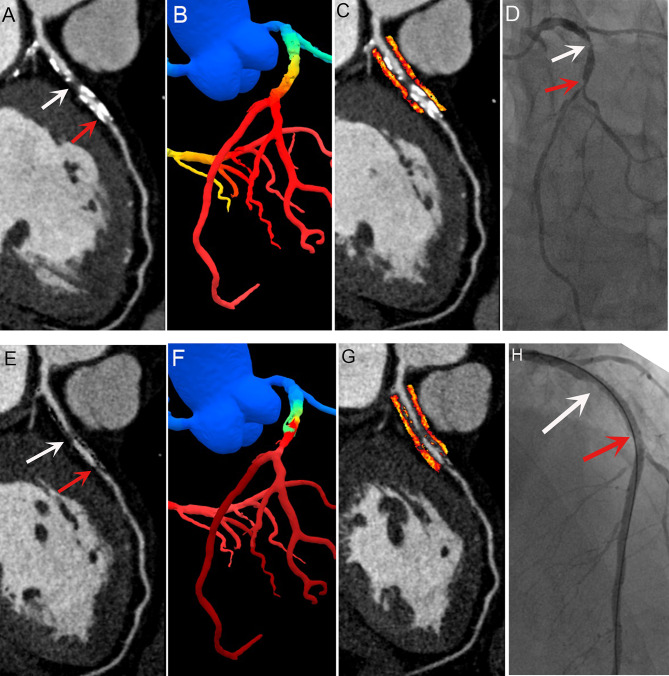
Background: Fractional flow reserve with computed tomography (FFR-CT) is influenced by calcified plaque artifacts, which can reduce its accuracy in predicting myocardial ischemia. Subtraction techniques can mitigate these artifacts, thereby enhancing diagnostic precision. However, the potential of subtraction FFR-CT and the pericoronary fat attenuation index (FAI) to improve the prediction of revascularization in patients with coronary artery disease (CAD) remains unclear. We aimed to evaluate the diagnostic performance of FFR-CT and pericoronary FAI in identifying the need for revascularization in patients with CAD.
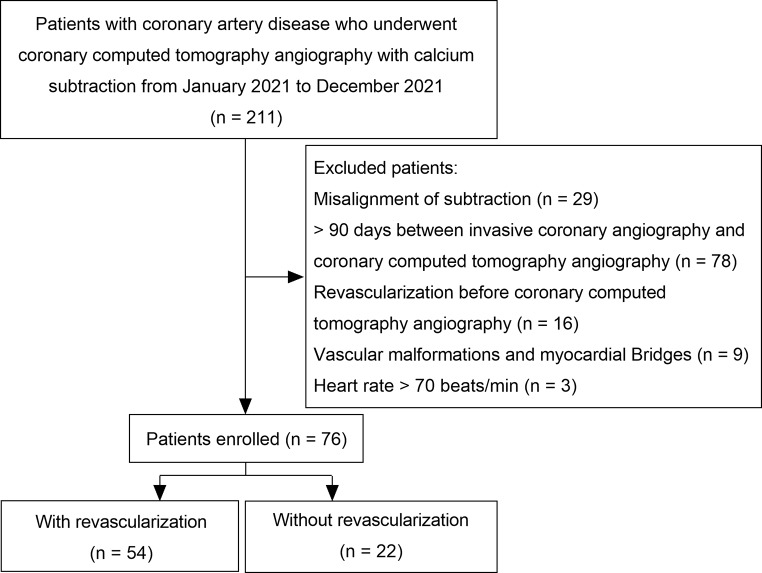
Methods: We retrospectively analyzed coronary computed tomography angiography (CCTA) data from 76 patients with CAD (142 branches) using both conventional and subtraction CCTA images. The diagnostic performance of FFR-CT and FAI in identifying revascularization needs was assessed using receiver operating characteristic curves.
Results: Among the 76 patients, 54 underwent revascularization. Patients who underwent revascularization had higher pericoronary FAI and lower FFR-CT values. Subtraction FFR-CT values were higher than those obtained using conventional methods. Models 4 (subtraction CCTA), 5 (Model 4 + subtraction FFR-CT), and 6 (Model 5 + subtraction FAI) showed significantly better diagnostic efficacy for revascularization needs than compared to the Models 1 (conventional CCTA), 2 (Model 1 + conventional FFR-CT), and 3 (Model 2 + conventional FAI) (all p < 0.05). In the subtraction models, Model 6 and 5 were significantly more effective than Models 4 (all p < 0.05). Additionally, when clinical variables (male, age, body mass index, hypertension, dyslipidemia, diabetes mellitus, and smoking) were incorporated into Models 3 and 6, the resulting Models 7 and 8 performed significantly better than Model 3 (all p < 0.05).
Conclusion: Subtraction techniques have significantly improved the efficacy of CCTA with FFR-CT in assessing the need for revascularization in patients with CAD. By integrating clinical variables, CCTA, FFR-CT, and pericoronary FAI, individualized therapeutic decisions for CAD patients can be further optimized.
Keywords: Coronary artery disease; Coronary computed tomography angiography; Fat attenuation index; Fractional flow reserve; Subtraction.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Tongji Medical College of Huazhong University of Science (February 1, 2020 /No. 2020-S336). The Ethics Committee of Tongji Medical College of Huazhong University of Science waived the requirement for informed consent. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Koo BK, Erglis A, Doh JH, et al. Diagnosis of ischemia-causing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms. Results from the prospective multicenter DISCover-FLOW (Diagnosis of Ischemia-Causing stenoses obtained via noninvasive fractional flow Reserve) study. J Am Coll Cardiol. 2011;58:1989–97. 10.1016/j.jacc.2011.06.066. - DOI - PubMed
-
- Oikonomou EK, Marwan M, Desai MY, et al. Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): a post-hoc analysis of prospective outcome data. Lancet. 2018;392:929–39. 10.1016/S0140-6736(18)31114-0. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
