

Heterogeneity in association of myocardial injury and mortality in sepsis or acute respiratory distress syndrome by subphenotype: a retrospective study
- PMID: 40826103
- PMCID: PMC12363128
- DOI: 10.1186/s13054-025-05613-2
Heterogeneity in association of myocardial injury and mortality in sepsis or acute respiratory distress syndrome by subphenotype: a retrospective study
Abstract
Rationale: Myocardial injury is common in acute respiratory distress syndrome (ARDS) and sepsis and associated with increased mortality. Two latent class analysis derived subphenotypes are associated with differential risk of mortality in these populations, though the association of troponin-I with mortality within each subphenotype is unknown.
Methods: The derivation (n = 597 in EARLI) and validation (n = 452 in VALID) cohorts consisted of patients with sepsis or ARDS admitted to the ICU and enrolled in two separate prospective observational studies. Patients with troponin-I measured between hospital presentation and within 24 h of ICU admission were included. A parsimonious classifier model using interleukin-8, soluble tumor necrosis factor receptor-1, and vasopressor use assigned patients to subphenotype. Association between peak troponin-I concentration and 60-day in-hospital mortality within each subphenotype was assessed through logistic regression adjusting for age, admission laboratory values, vasopressor use, invasive ventilation use, and cardiac comorbidities.
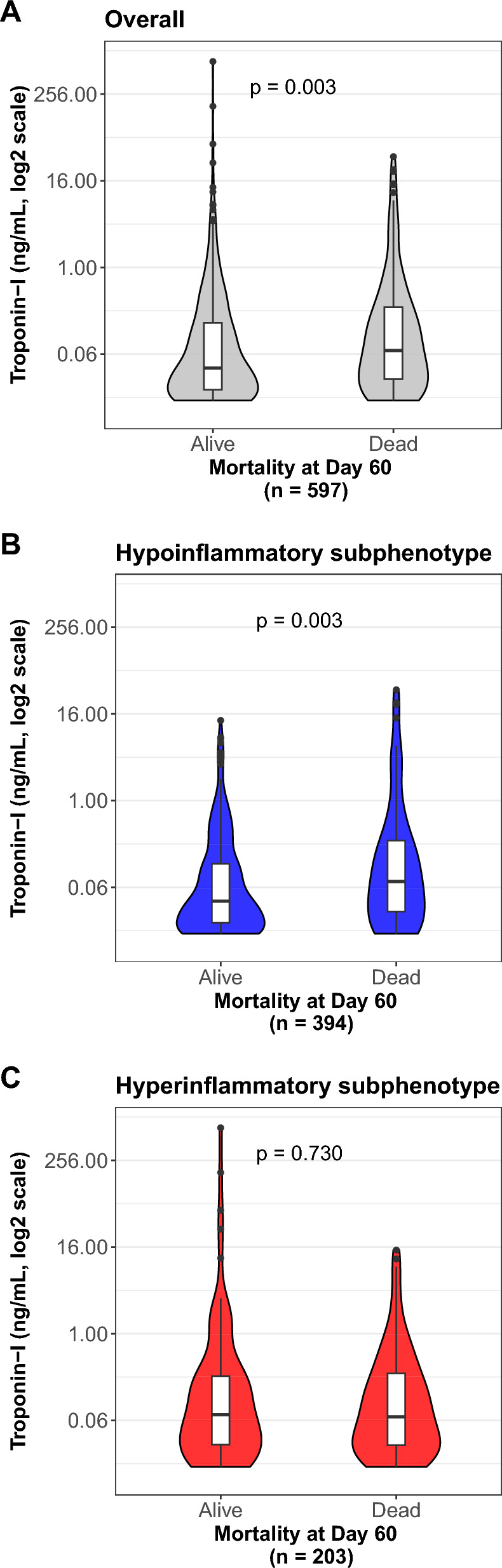
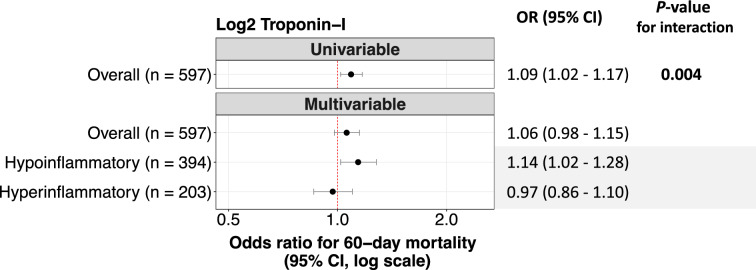
Results: Median peak troponin-I was significantly higher in the hyperinflammatory vs hypoinflammatory subphenotype in both cohorts (0.07 vs 0.04 ng/mL and 0.17 vs 0.07 ng/mL, both p < 0.05). The association between peak troponin-I and mortality differed between inflammatory subphenotypes (p-interaction 0.004, EARLI). In EARLI, each doubling of peak troponin-I was associated with increased adjusted odds of 60-day mortality (aOR 1.14, 95% CI 1.02-1.28) in the hypoinflammatory subphenotype only. These findings were corroborated in VALID (aOR 1.11, 95% CI 1.03-1.21 in hypoinflammatory).
Conclusions: Admission peak troponin-I is significantly associated with 60-day mortality in patients with sepsis or ARDS. This association was distinctly driven by the hypoinflammatory subphenotype.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: EARLI was approved by the UCSF institutional review board (IRB, #10-02852) and VALID by the Vanderbilt IRB (#051065). Patients or surrogates were consented for participation when possible. Competing interests: The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
