

JNK pathway suppression mediates insensitivity to combination endocrine therapy and CDK4/6 inhibition in ER+ breast cancer
- PMID: 40826108
- PMCID: PMC12363127
- DOI: 10.1186/s13046-025-03466-9
JNK pathway suppression mediates insensitivity to combination endocrine therapy and CDK4/6 inhibition in ER+ breast cancer
Abstract
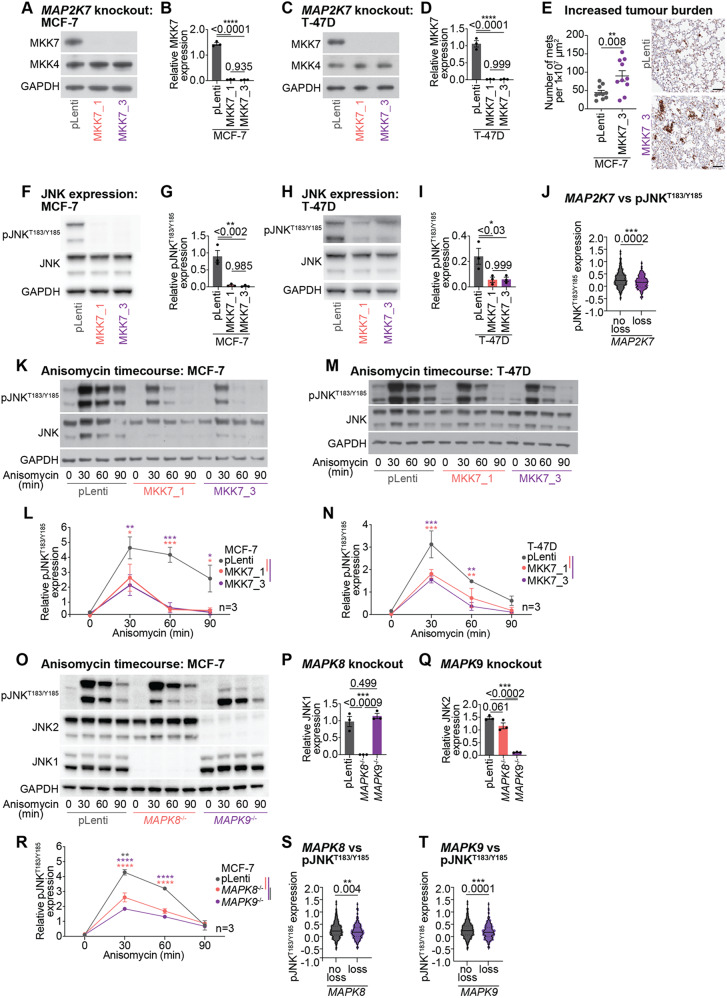
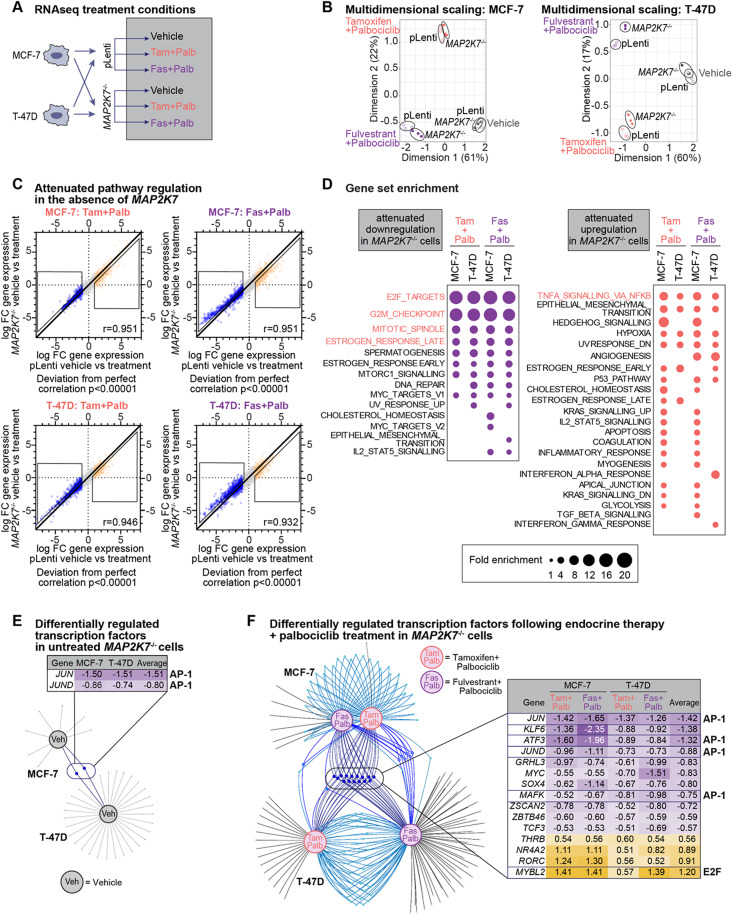
CDK4/6 inhibitors in combination with endocrine therapy are now used as front-line treatment for patients with estrogen-receptor positive (ER+) breast cancer. While this combination improves overall survival, the mechanisms of disease progression remain poorly understood. Here, we performed unbiased genome-wide CRISPR/Cas9 knockout screens using endocrine sensitive ER+ breast cancer cells to identify novel drivers of resistance to combination endocrine therapy (tamoxifen) and CDK4/6 inhibitor (palbociclib) treatment. Our screens identified the inactivation of JNK signalling, including loss of the kinase MAP2K7, as a key driver of drug insensitivity. We developed multiple CRISPR/Cas9 knockout ER+ breast cancer cell lines (MCF-7 and T-47D) to investigate the effects of MAP2K7 and downstream MAPK8 and MAPK9 loss. MAP2K7 knockout increased metastatic burden in vivo and led to impaired JNK-mediated stress responses, as well as promoting cell survival and reducing senescence entry following endocrine therapy and CDK4/6 inhibitor treatment. Mechanistically, this occurred via loss of the AP-1 transcription factor c-JUN, leading to an attenuated response to combination endocrine therapy plus CDK4/6 inhibition. Furthermore, analysis of clinical datasets found that inactivation of the JNK pathway was associated with increased metastatic burden, and low pJNKT183/Y185 activity correlated with a poorer response to systemic endocrine and CDK4/6 inhibitor therapies in both early-stage and metastatic ER+ breast cancer cohorts. Overall, we demonstrate that suppression of JNK signalling enables persistent growth during combined endocrine therapy and CDK4/6 inhibition. Our data provides the pre-clinical rationale to stratify patients based on JNK pathway activity prior to receiving combination endocrine therapy and CDK4/6 inhibition.
Keywords: CDK4/6 inhibition; ER+ breast cancer; Endocrine therapy; JNK signalling; Palbociclib.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All animal work was performed in compliance with the Australian Code of Practice for the Care and Use of Animals for Scientific Purposes (National Health and Medical Research Council). The protocol and study end points were approved by the St. Vincent’s Health Precinct and GIMR Animal Ethics Committee (ARA 21/09). Consent for publication: N/A. Competing interests: E. L provides advisory board services to AstraZeneca, Gilead, Lilly, MDS, Novartis, Pfizer, Roche, and received royalties from Walter and Eliza Hall Institute.
Figures




References
-
- Finn RS, et al. Palbociclib and letrozole in advanced breast Cancer. N Engl J Med. 2016;375:1925–36. 10.1056/NEJMoa1607303. - PubMed
-
- Hortobagyi GN, et al. Ribociclib as First-Line therapy for HR-Positive, advanced breast Cancer. N Engl J Med. 2016;375:1738–48. 10.1056/NEJMoa1609709. - PubMed
-
- Goetz MP, et al. MONARCH 3: abemaciclib as initial therapy for advanced breast cancer. J Clin Oncology: Official J Am Soc Clin Oncol. 2017;35:3638–46. 10.1200/JCO.2017.75.6155. - PubMed
-
- Slamon D, et al. Ribociclib plus fulvestrant for postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in the phase III randomized MONALEESA-3 trial: updated overall survival. Ann Oncol. 2021;32:1015–24. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
