

Prognostic value of triglyceride-glucose index combined with stress hyperglycemia ratio for all-cause mortality in critically ill patients with stroke
- PMID: 40826360
- PMCID: PMC12362854
- DOI: 10.1186/s12933-025-02901-7
Prognostic value of triglyceride-glucose index combined with stress hyperglycemia ratio for all-cause mortality in critically ill patients with stroke
Abstract
Background: The triglyceride-glucose (TyG) index and stress hyperglycemia ratio (SHR) are emerging biomarkers in cerebrovascular diseases, but their combined prognostic value for mortality in patients with critically ill stroke remains unexplored. This study, based on a cohort of critically ill patients with stroke, aims to investigate the prognostic value of the combined TyG index and SHR in predicting all-cause mortality at multiple time points in this high-risk population.
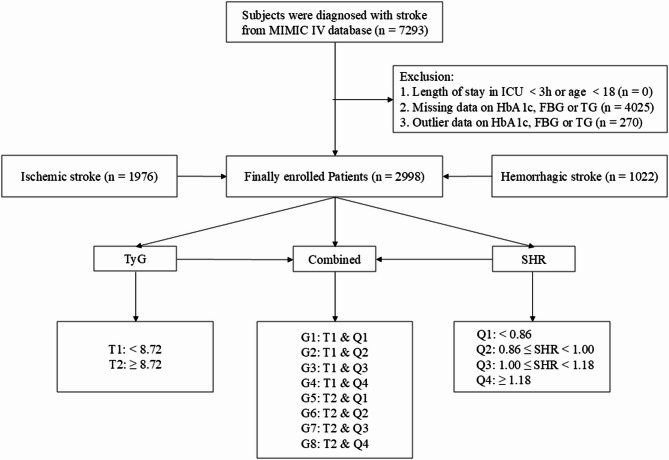
Methods: Based on the Medical Information Mart for Intensive Care (MIMIC)-IV database, 2998 critically ill patients with stroke requiring intensive care unit (ICU) admission were included. Patients were stratified into 8 groups based on the median of the TyG index and the quartiles of the SHR. The primary outcomes were 30-day and 365-day all-cause mortality; the secondary outcomes included 90-day and 180-day mortality. Cox proportional hazards regression models, restricted cubic splines (RCS) curves, subgroup analyses, and mediation analyses were employed to assess associations between the combined TyG index and SHR with all-cause mortality.
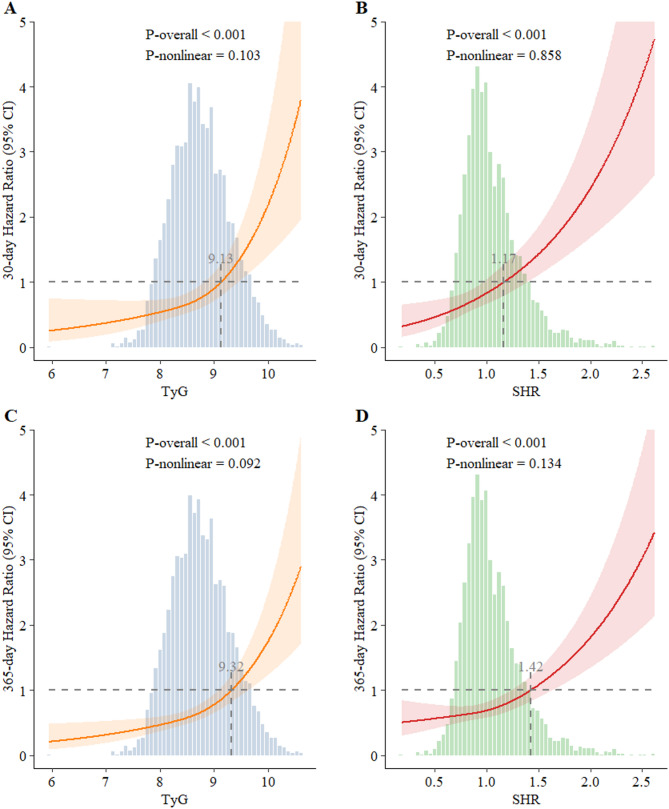
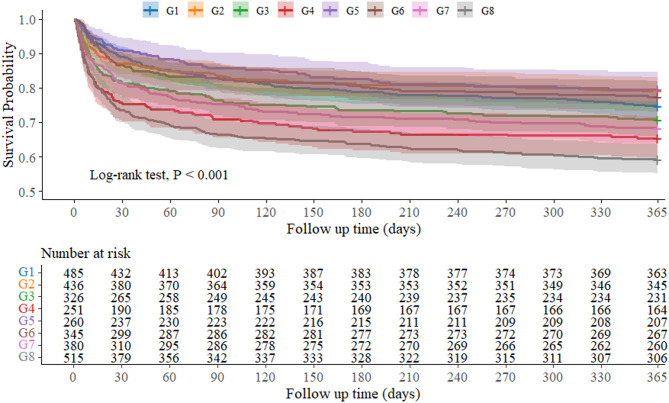
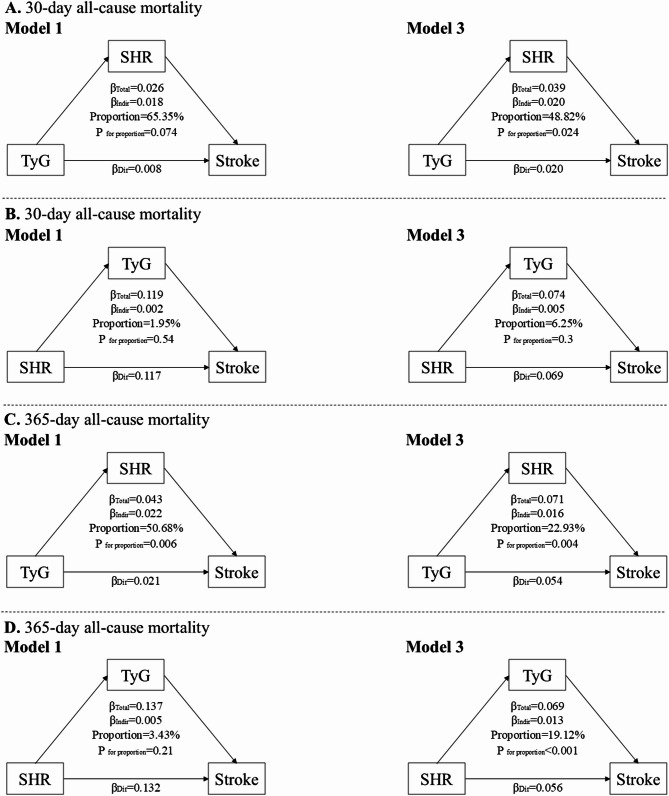
Results: The cohort had a median age of 72.63 years (IQR 61.27-82.69 years), with 51.33% male (1539/2998). Fully adjusted Cox proportional hazards models showed that compared to the reference group (TyG < 8.72 and SHR < 0.86), patients with TyG ≥ 8.72 and SHR ≥ 1.18 had the highest mortality risk (30-day HR 2.481, 95% CI 1.767-3.485; 365-day HR 1.954, 95% CI 1.532-2.493). RCS analysis confirmed linear positive correlations between the TyG index, SHR, and mortality at all time points (all P for non-linearity > 0.05). Subgroup analyses further demonstrated consistent associations between the combined TyG index and SHR on 30-day and 365-day all-cause mortality. Mediation analysis revealed that the highest SHR significantly mediated the association between high TyG and mortality in these patients (30-day mediation proportion: 48.82%, P = 0.024; 365-day: 22.93%, P = 0.004).
Conclusion: The combination of high TyG (≥ 8.72) and elevated SHR (≥ 1.18) is significantly associated with increased short- and long-term mortality in critically ill patients with stroke. Integrated metabolic monitoring and early intervention targeting at these biomarkers may improve their prognosis.
Keywords: MIMIC-IV; Mortality; Stress hyperglycemia ratio; Stroke; Triglyceride-glucose index.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study utilized a publicly available, de-identified database (MIMIC-IV) that had received pre-existing institutional review board (IRB) approval. The IRB at the Beth Israel Deaconess Medical Center (protocol 2001-P-001699/14) and Massachusetts Institute of Technology (protocol 0403000206) approved the data collection and research use of this database, and granted waiver of informed consent. All procedures and analyses complied with applicable ethical guidelines and regulations. Consent for publication: No applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Association between trajectory of triglyceride-glucose index and all-cause mortality in critically ill patients with atrial fibrillation: a retrospective cohort study.Cardiovasc Diabetol. 2025 Jul 10;24(1):278. doi: 10.1186/s12933-025-02838-x. Cardiovasc Diabetol. 2025. PMID: 40640797 Free PMC article.
-
Association between triglyceride-glucose index and mortality in critically ill patients with atrial fibrillation: a retrospective cohort study.Cardiovasc Diabetol. 2025 Mar 24;24(1):138. doi: 10.1186/s12933-025-02697-6. Cardiovasc Diabetol. 2025. PMID: 40128768 Free PMC article.
-
Association between triglyceride-glucose-body mass index and adverse prognosis in elderly patients with severe heart failure and type 2 diabetes: a retrospective study based on the MIMIC-IV database.Cardiovasc Diabetol. 2025 Jul 24;24(1):299. doi: 10.1186/s12933-025-02870-x. Cardiovasc Diabetol. 2025. PMID: 40707996 Free PMC article.
-
Does diabetes status modify the association between the triglyceride-glucose index and major adverse cardiovascular events in patients with coronary heart disease? A systematic review and meta-analysis of longitudinal cohort studies.Cardiovasc Diabetol. 2025 Aug 4;24(1):317. doi: 10.1186/s12933-025-02890-7. Cardiovasc Diabetol. 2025. PMID: 40760488 Free PMC article.
-
The impact of triglyceride-glucose index on ischemic stroke: a systematic review and meta-analysis.Cardiovasc Diabetol. 2023 Jan 6;22(1):2. doi: 10.1186/s12933-022-01732-0. Cardiovasc Diabetol. 2023. PMID: 36609319 Free PMC article.
References
-
- Chen Y, Yang Z, Liu Y, Li Y, Zhong Z, McDowell G, et al. Exploring the prognostic impact of triglyceride-glucose index in critically ill patients with first-ever stroke: insights from traditional methods and machine learning-based mortality prediction. Cardiovasc Diabetol. 2024;23(1):443. - PMC - PubMed
-
- Lavados PM, Hoffmeister L, Moraga AM, Vejar A, Vidal C, Gajardo C, et al. Incidence, risk factors, prognosis, and health-related quality of life after stroke in a low-resource community in Chile (ÑANDU): a prospective population-based study. Lancet Glob Health. 2021;9(3):e340–51. - PubMed
-
- Jin M, Bao Z, Hong X, He S, Gao F. The prognostic value of the stress hyperglycemia ratio for all-cause mortality in stroke patients with diabetes or prediabetes. J Diabetes Complicat. 2025;39(4):108979. - PubMed
Grants and funding
- 202205230031-3/Postdoctoral Research Initiation Grant
- 2022A1515110139/Guangdong Basic and Applied Research Foundation
- 2021A1515110873/Guangdong Basic and Applied Research Foundation
- 009-510858038/SUMC Scientific Research Initiation Grant
- 20210930038/First Affiliated Hospital of SUMC Scientific Research Initiation Grant
LinkOut - more resources
Full Text Sources
