

Fixation versus revision arthroplasty for Unified Classification System type B periprosthetic fractures around cemented polished tapered femoral components : a systematic review and meta-analysis
- PMID: 40827095
- PMCID: PMC12362029
- DOI: 10.1302/2633-1462.68.BJO-2025-0123
Fixation versus revision arthroplasty for Unified Classification System type B periprosthetic fractures around cemented polished tapered femoral components : a systematic review and meta-analysis
Abstract
Aims: Periprosthetic femoral fractures (PFF) around hip arthroplasty implants are increasingly common, often occurring in frail elderly patients. Polished taper-slip (PTS) cemented femoral components are commonly used and have been associated with increased PFF rates compared with other cemented femoral component types. In managing Unified Classification System (UCS) type B fractures around PTS stems, surgical treatment options include open reduction and internal fixation (ORIF) and revision arthroplasty (RA), but there is limited evidence comparing these.
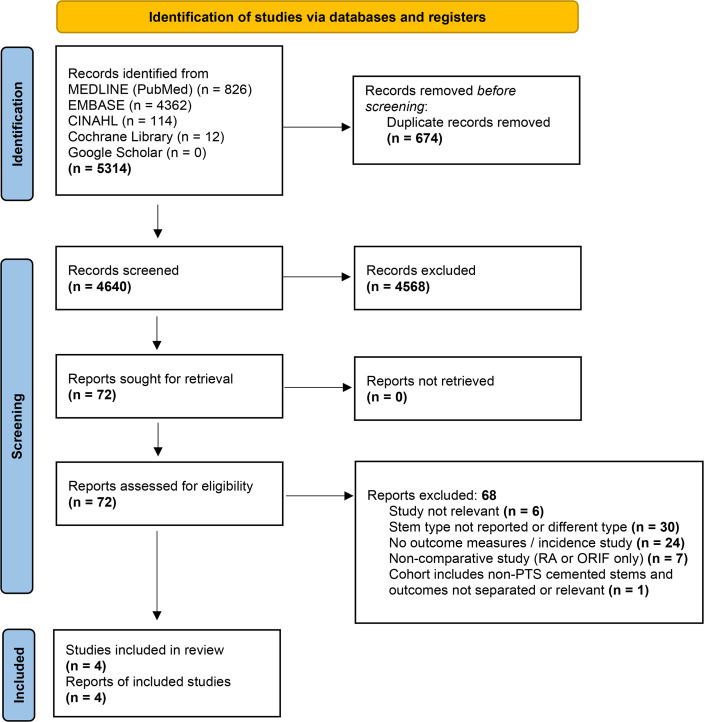
Methods: A systematic review and meta-analysis was undertaken. Results from database searching were screened and data were extracted by two authors independently. Reoperation was the primary outcome measure, and the secondary outcome measures included mortality, blood transfusion requirements, and length of stay.
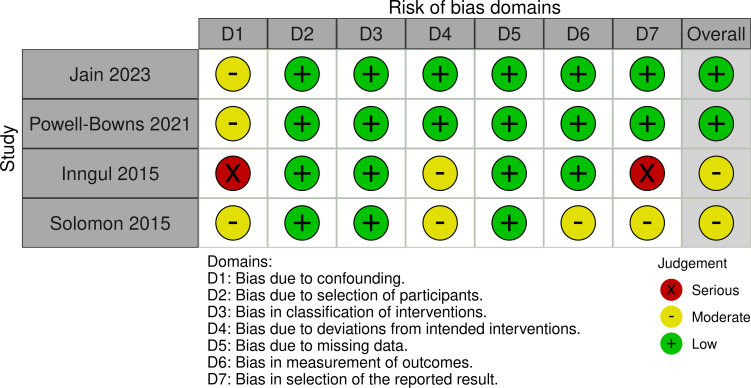
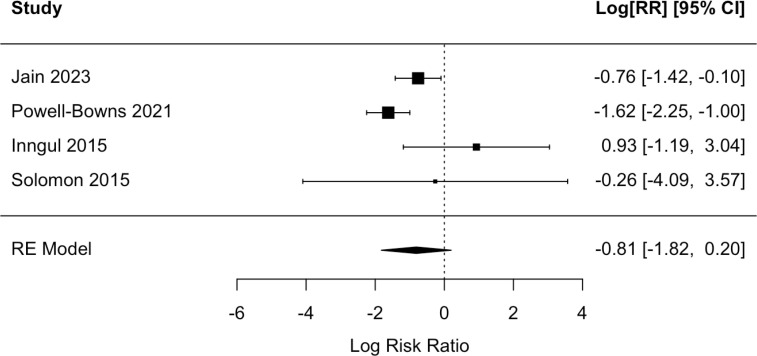
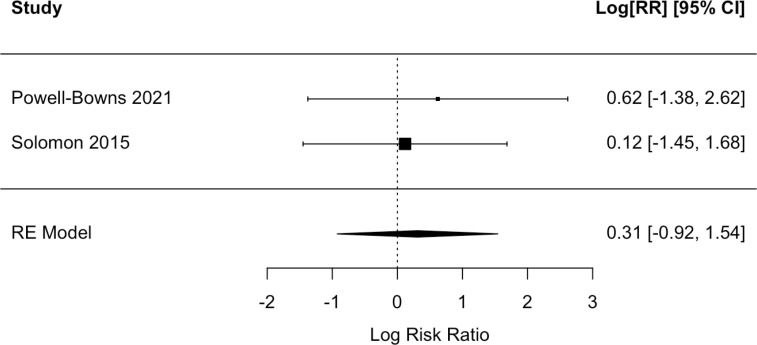
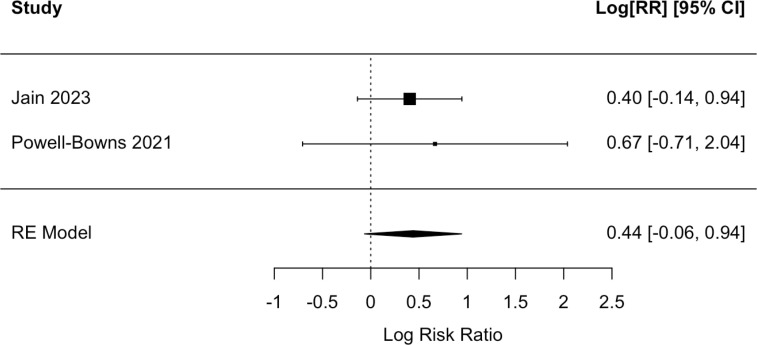
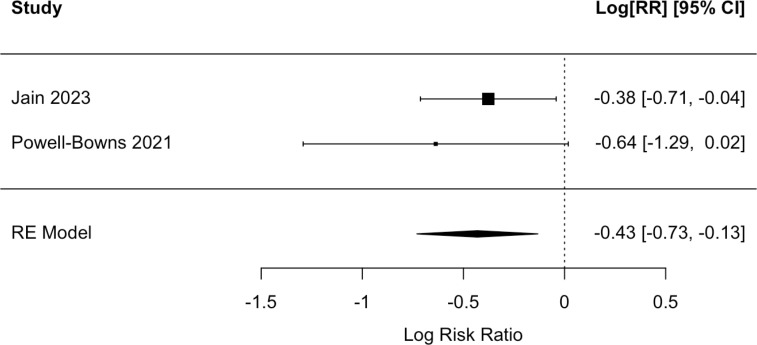
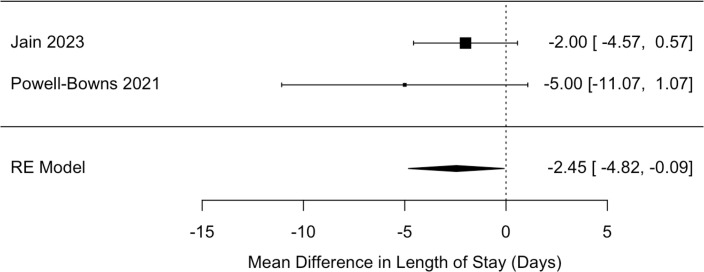
Results: There were 4,640 unique results, and four comparative studies were included in the final analysis. These were published between 2015 to 2023, totalling 539 patients, with 339 treated with ORIF and 200 treated with RA. There was a signal for a clinically large, but not statistically significant, benefit of ORIF compared with RA in reoperation risk (risk ratio (RR) 0.444; 95% CI 0.162 to 1.218; p = 0.115), with an absolute risk reduction of 9.15%. There was also a non-significant signal for increased mortality in the ORIF group at both 90 days and one year. ORIF was associated with a significant decrease in blood transfusion requirements (RR 0.65; 95% CI 0.482 to 0.876; p = 0.005), with an absolute risk reduction of 14.07%. There was also a significant decrease in length of stay following ORIF (mean reduction 2.45 days; 95% CI 0.09 to 4.82; p = 0.042).
Conclusion: Fixation alone is associated with significantly reduced length of stay and blood transfusion, and also with a trend towards reduced reoperation and increased mortality, which may reflect a frailer patient group that receive this treatment, but neither of these findings reached statistical significance. Fixation may have benefits when applied in suitable cases.
© 2025 Walters et al.
Conflict of interest statement
None declared.
Figures
Similar articles
-
What Is the Cumulative Incidence of Femoral Stem Revision and Stem Complication in Cemented and Uncemented Hip Arthroplasty for Proximal Femoral Metastatic Bone Disease?Clin Orthop Relat Res. 2025 Jun 10;483(9):1652-64. doi: 10.1097/CORR.0000000000003541. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40522275
-
Are There Differences in Performance Among Femoral Stem Brands Utilized in Cementless Hemiarthroplasty for Treatment of Geriatric Femoral Neck Fractures?Clin Orthop Relat Res. 2025 Feb 1;483(2):253-264. doi: 10.1097/CORR.0000000000003222. Epub 2024 Aug 15. Clin Orthop Relat Res. 2025. PMID: 39158389
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Surgical interventions for treating intracapsular hip fractures in older adults: a network meta-analysis.Cochrane Database Syst Rev. 2022 Feb 14;2(2):CD013404. doi: 10.1002/14651858.CD013404.pub2. Cochrane Database Syst Rev. 2022. PMID: 35156192 Free PMC article.
-
Surgical versus non-surgical interventions for displaced intra-articular calcaneal fractures.Cochrane Database Syst Rev. 2023 Nov 7;11(11):CD008628. doi: 10.1002/14651858.CD008628.pub3. Cochrane Database Syst Rev. 2023. PMID: 37933733 Free PMC article.
References
-
- National Joint Registry Hips - All procedures - Activity. 2024. [8 August 2025]. https://reports.njrcentre.org.uk/hips-all-procedures-activity date last. accessed.
-
- Royal College of Physicians . London: RCP; 2023. [ August 2025]. 15 Years of Quality Improvement: The 2023 National Hip Fracture Database Report on 2022.https://www.nhfd.co.uk/20/hipfractureR.nsf/docs/2023Report date last. accessed.
LinkOut - more resources
Full Text Sources
