

Unusual presentation of an infected Meckel's diverticulum with umbilical perforation and granulomatous lesion in a young Adult: A rare case report from a resource-constrained setting
- PMID: 40829404
- PMCID: PMC12395488
- DOI: 10.1016/j.ijscr.2025.111841
Unusual presentation of an infected Meckel's diverticulum with umbilical perforation and granulomatous lesion in a young Adult: A rare case report from a resource-constrained setting
Abstract
Background: Meckel's diverticulum (MD), a congenital anomaly of the gastrointestinal tract, affects approximately 2 % of the population, but complications occur in only 4-6 % of cases. Symptomatic MD is typically seen in children, with adult presentations being rare and often incidental. Umbilical complications related to persistent vitelline duct remnants are extremely uncommon in adults.
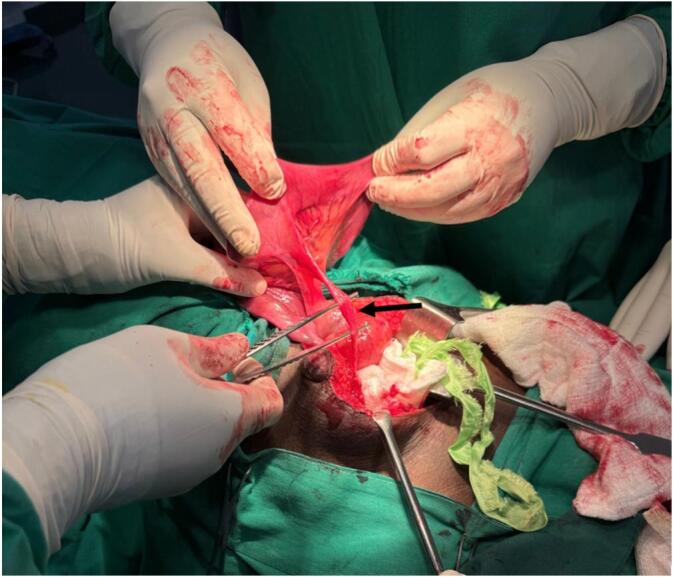
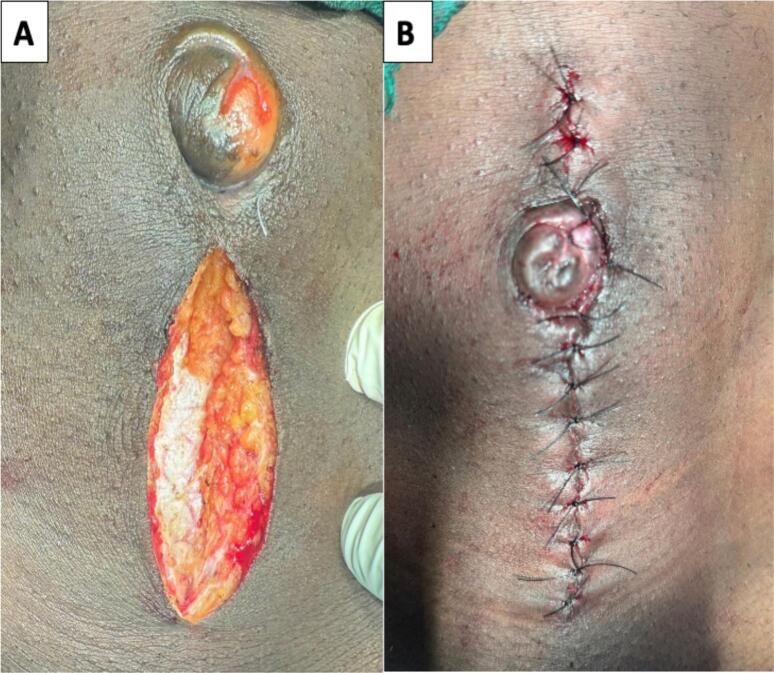
Case presentation: A 21-year-old-male without previous abdominal symptoms presented with a two-year history of dull periumbilical pain, gradually progressing to purulent umbilical discharge, low-grade fever, a small sinus opening, and granulomatous tissue. Laboratory investigations including CBC, CRP, and liver/renal panels were normal. Ultrasound revealed a hypoechoic tract from the umbilicus to the pelvis, suggestive of an infected urachal remnant. Exploratory laparotomy revealed a 2-inch inflamed Meckel's diverticulum located 65 cm from the ileocecal valve, connected to the umbilicus by a fibrous tract. Diverticulectomy, excision of the tract and granuloma, and umbilicoplasty were performed. Histopathology confirmed MD with chronic inflammation and no ectopic mucosa. The postoperative course was uneventful.
Discussion: This case illustrates a rare adult complication of MD presenting as an umbilical sinus with granulomatous changes, mimicking a urachal anomaly. While adult MD typically presents with bleeding, obstruction, or inflammation, umbilical fistulation is rarely reported in adults. Early surgical exploration was essential for accurate diagnosis and treatment.
Conclusion: Infected MD with umbilical perforation and granulomatous tissue is exceptionally rare in adults. It should be considered in the differential diagnosis of persistent umbilical discharge. Surgical exploration can provide definitive diagnosis and curative treatment, particularly in resource-limited settings.
Keywords: Case report; Diverticulectomy; Granulomatous lesion; Meckel's diverticulum; Umbilical perforation; Vitelline duct remnant.
Copyright © 2025 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare no conflict of interest.
Figures




Similar articles
-
Perforated Meckel's diverticulum mimicking appendicitis in a 64-year-old male: a case report and comparative analysis from a resource-limited setting.Ann Med Surg (Lond). 2025 Jul 14;87(9):6096-6100. doi: 10.1097/MS9.0000000000003590. eCollection 2025 Sep. Ann Med Surg (Lond). 2025. PMID: 40901123 Free PMC article.
-
Perforated meckel's diverticulum misdiagnosed as a urinary tract infection in an 11-year-old adolescent: case report of a rare differential diagnosis.Patient Saf Surg. 2025 Jul 3;19(1):20. doi: 10.1186/s13037-025-00443-1. Patient Saf Surg. 2025. PMID: 40611290 Free PMC article.
-
Laparoscopic management of small bowel obstruction due to a mesodiverticular band of a Meckel's diverticulum: A case report.Int J Surg Case Rep. 2025 Aug;133:111643. doi: 10.1016/j.ijscr.2025.111643. Epub 2025 Jul 9. Int J Surg Case Rep. 2025. PMID: 40644979 Free PMC article.
-
Coexistence of cecal duplication cyst and Meckel's diverticulum presenting as intussusception in a malnourished child a case report with literature review.BMC Pediatr. 2025 Jul 1;25(1):479. doi: 10.1186/s12887-025-05823-1. BMC Pediatr. 2025. PMID: 40597078 Free PMC article. Review.
-
Systematic review of epidemiology, presentation, and management of Meckel's diverticulum in the 21st century.Medicine (Baltimore). 2018 Aug;97(35):e12154. doi: 10.1097/MD.0000000000012154. Medicine (Baltimore). 2018. PMID: 30170459 Free PMC article.
References
-
- Yamaguchi M., Takeuchi S., Awazu S. Meckel’s diverticulum: investigation of 600 patients in Japanese literature. Am. J. Surg. 1978;136(2):247–249. - PubMed
-
- St. George T.J., Liu E., Golub R., et al. The rule of 2s: meckel diverticulum’s epidemiology unchanged after years of study. J. Gastroenterol. Hepatol. 2016;31(Suppl. 2):16–19.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
