

Exploring sex differences in mortality among acute myocardial infarction
- PMID: 40829892
- PMCID: PMC12366619
- DOI: 10.1136/openhrt-2025-003517
Exploring sex differences in mortality among acute myocardial infarction
Abstract
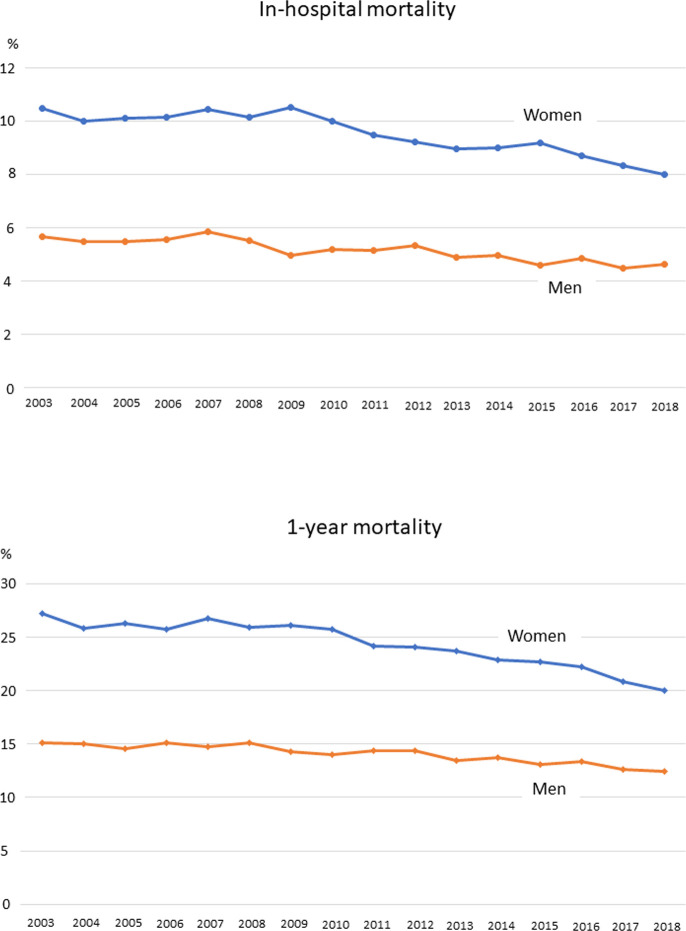
Background: Women with acute myocardial infarction (AMI) experience higher mortality rates than men. This disparity is influenced by factors such as older age, greater comorbidity burden, atypical symptom presentation and delays in treatment. This study analysed patients with AMI (2003-2018) from the Lombardy Health Database (Italy) to examine sex differences in in-hospital and 1-year mortality and the role of age, percutaneous coronary intervention (PCI) and postdischarge therapy.
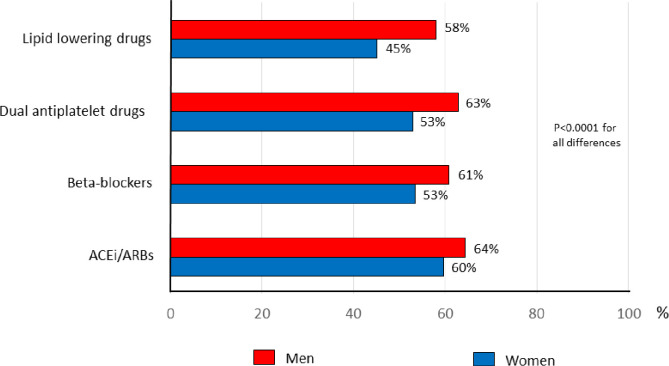
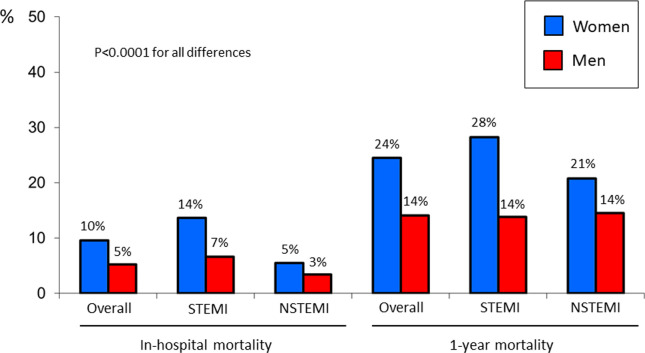
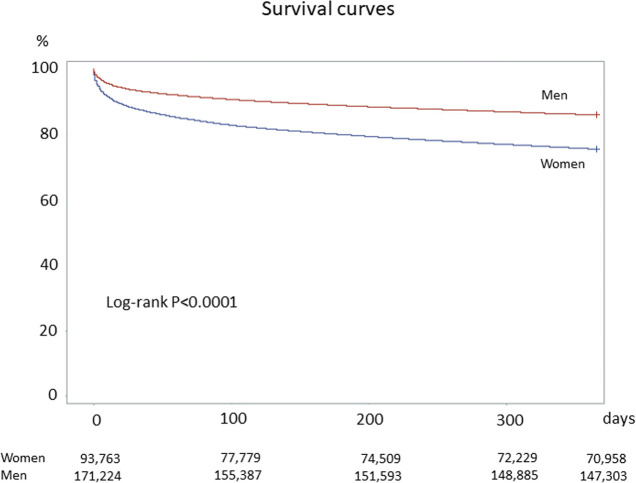
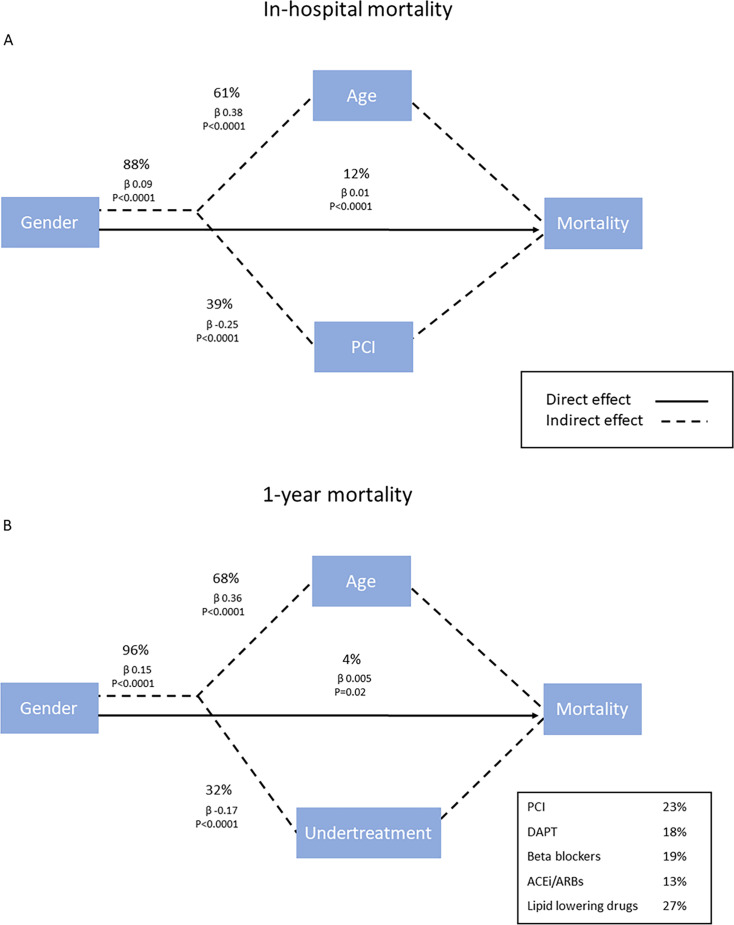
Methods and results: Among 263 564 patients with AMI (93 363 women, 170 201 men), primary and secondary endpoints were in-hospital and 1-year mortality, respectively. Path analysis evaluated the direct and indirect effects of sex on outcomes, incorporating age, PCI and postdischarge therapy as mediators. Women had higher in-hospital (10% vs 5%; p<0.0001) and 1-year mortality (24% vs 14%; p<0.0001) but were less likely to receive PCI (40% vs 61%; p<0.0001) and postdischarge therapy (dual antiplatelet therapy 53% vs 63%; ACE inhibitors/angiotensin receptor blockers 60% vs 64%; beta blockers 53% vs 61%; lipid-lowering drugs 45% vs 58%; p<0.0001 for all differences). After adjusting for age, major comorbidities, PCI and postdischarge treatment, mortality differences were no longer significant (adjusted OR 1.04; 95% CI 0.99 to 1.07 for in-hospital mortality) or even reversed (adjusted HR 0.94; 95% CI 0.92 to 0.96 for 1-year mortality). Path analysis showed that female sex directly contributed 12% to in-hospital mortality and 4% to 1-year mortality, while age and undertreatment accounted for most of the disparity (88% and 96%, respectively).
Conclusion: Women with AMI face higher mortality largely due to older age and undertreatment during hospitalisation and after discharge. Addressing these gaps could improve outcomes.
Keywords: Epidemiology; Myocardial Infarction; Percutaneous Coronary Intervention.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Sex differences in myocardial infarction care and outcomes: a longitudinal Scottish National Data-Linkage Study.Eur J Prev Cardiol. 2025 Jun 3;32(8):696-707. doi: 10.1093/eurjpc/zwae333. Eur J Prev Cardiol. 2025. PMID: 39592008
-
Preoperative coronary interventions for preventing acute myocardial infarction in the perioperative period of major open vascular or endovascular surgery.Cochrane Database Syst Rev. 2024 Jul 3;7(7):CD014920. doi: 10.1002/14651858.CD014920.pub2. Cochrane Database Syst Rev. 2024. PMID: 38958136 Free PMC article.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Outcomes of Percutaneous Coronary Intervention in Nonagenarians in the United States.Catheter Cardiovasc Interv. 2025 Jul;106(1):250-257. doi: 10.1002/ccd.31538. Epub 2025 Apr 16. Catheter Cardiovasc Interv. 2025. PMID: 40241276
-
Indobufen versus aspirin after percutaneous coronary intervention in elderly patients with acute coronary syndrome.BMC Cardiovasc Disord. 2025 Jul 7;25(1):495. doi: 10.1186/s12872-025-04843-0. BMC Cardiovasc Disord. 2025. PMID: 40619357 Free PMC article.
References
-
- Lee CY, Liu KT, Lu HT, et al. Sex and gender differences in presentation, treatment and outcomes in acute coronary syndrome, a 10 year study from a multi-ethnic Asian population: The Malaysian National Cardiovascular Disease Database-Acute Coronary Syndrome (NCVD-ACS) registry. PLoS One. 2021;16:e0246474. doi: 10.1371/journal.pone.0246474. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous