

Integrated molecular and clinical characterization of pulmonary large cell neuroendocrine carcinoma
- PMID: 40830141
- PMCID: PMC12365225
- DOI: 10.1038/s41467-025-63091-0
Integrated molecular and clinical characterization of pulmonary large cell neuroendocrine carcinoma
Abstract
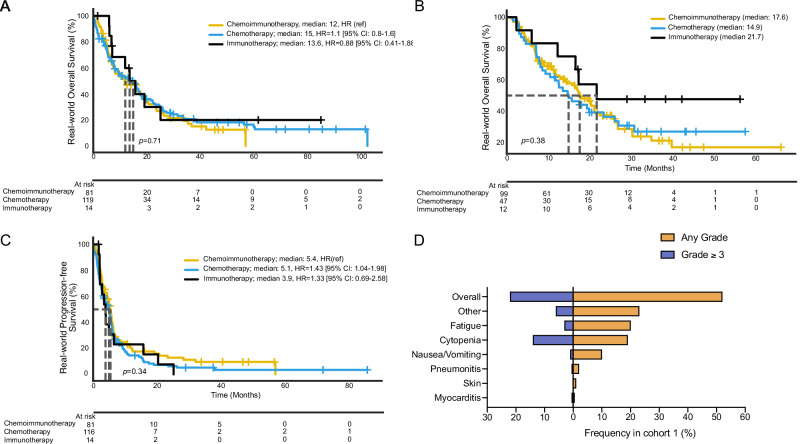
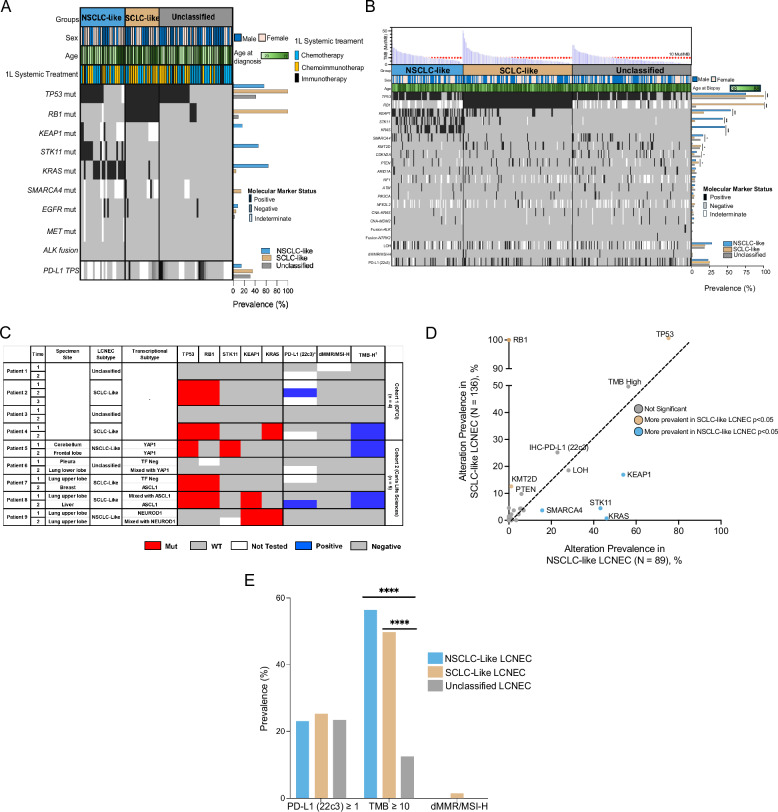
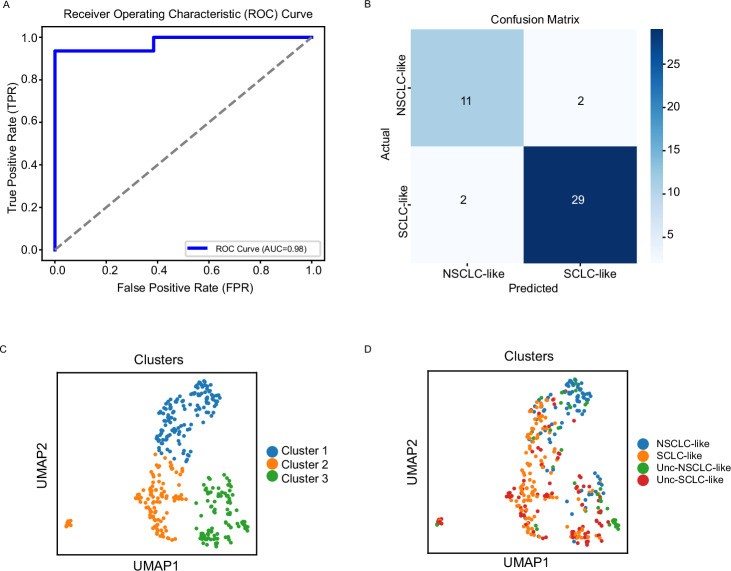
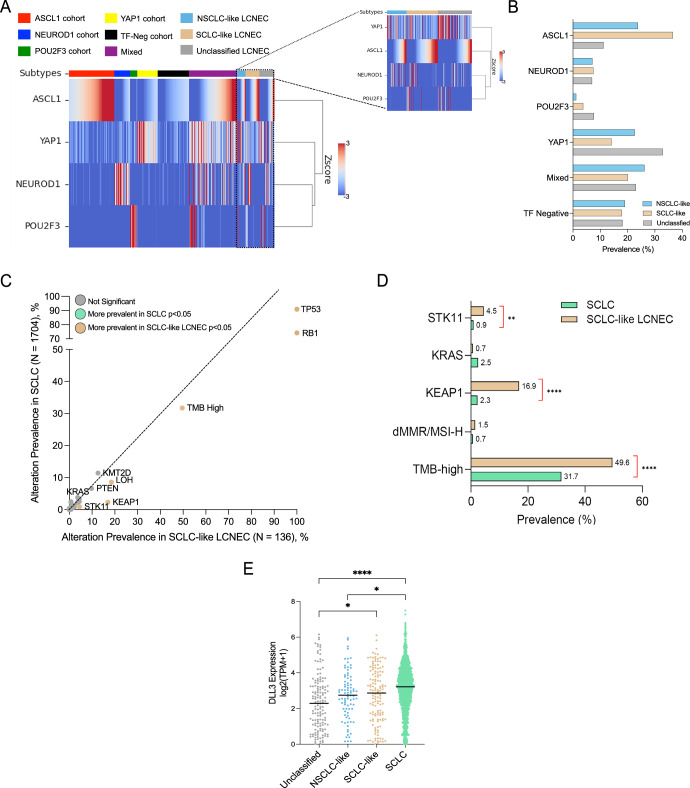
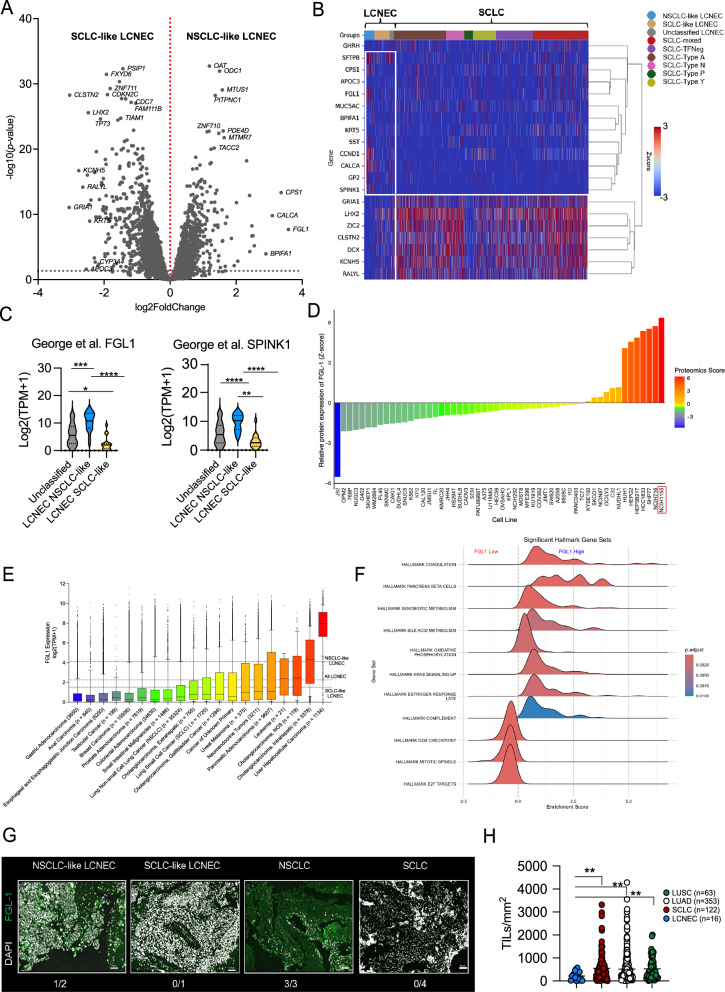
Pulmonary large cell neuroendocrine carcinoma (LCNEC) is a rare, aggressive lung tumor marked by significant molecular heterogeneity. In a study of 590 patients across two independent cohorts, we observe comparable overall survival across treatment regimens (chemotherapy, chemoimmunotherapy, immunotherapy) without unexpected adverse events. Genomic analysis identifies distinct non-small cell lung cancer-like (NSCLC-like, KEAP1, KRAS, STK11 mutations) and SCLC-like (RB1, TP53 mutations) LCNEC subtypes, with 80% aligning with SCLC transcriptional profiles. Serial sampling reveals stable mutational but shifting transcriptomic landscapes over time. Here we show, elevated FGL-1 (a LAG-3 ligand) and SPINK1 expression in NSCLC-like LCNECs, and higher levels of DLL3 in SCLC-like LCNECs. Immunofluorescence confirms FGL-1 expression in NSCLC-like LCNECs, and H&E slide analyses indicates fewer tumor-infiltrating lymphocytes in LCNECs versus other lung cancers. These findings highlight LCNEC's distinct immunogenomic profile, supporting future investigations into LAG-3, SPINK1, and DLL3-targeted therapies.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: A.H.N.: honoraria: the Korean Society of Medical Oncology, TEMPUS, OncLive, Oklahoma University, Targeted Oncology; travel compensation: Korean Society of Medical Oncology, American Association for Cancer Research; consultation fees: Guidepoint Global, Putnam Associates, Capvision; compensation from Outlier.ai to provide feedback on data analysis tools, AI development; Equity in Revolution Medicine, Summit Therapeutics. M.G.E. receives full-time employment, travel/speaking expenses, and stock/stock options from Caris Life Sciences. A.C.C.: advisory boards: AbbVie, Amgen, BI, Merck, Jazz, and Research funding: Zai Labs. D.J.P.: Lecture fees: Bayer Healthcare, AstraZeneca, EISAI, Bristol Myers Squibb, Roche, Ipsen, OncLive; Travel expenses: Bristol Myers Squibb, Roche, Bayer Healthcare; Consulting fees: Mina Therapeutics, Boeringer Ingelheim, Ewopharma, EISAI, Ipsen, Roche, H3B, AstraZeneca, DaVolterra, Starpharma, Boston Scientific, Mursla, Avammune Therapeutics, LiFT Biosciences, Exact Sciences; Research funding (to institution): MSD, BMS, GSK, EISAI. N.A.: No conflicts to declare. P.R. reports travel support from AstraZeneca, MSD, BMS, and Kiowa Kirin outside the submitted work. M.R. received lecture fees from AstraZeneca. F.A.-L.: Research PI (AZ, Alira Health). A.I.V. received consulting honorarium from AstraZeneca, AbbVie, Janssen, Regeneron, Merus, and Novocure. T.A.: Employee of Caris Life Sciences. J.Z. reported the following: Grants/Contracts: AbbVie, AstraZeneca, BeiGene, BridgeBio, Genentech, Hengrui Therapeutics, InnoCare Pharma, Janssen, Kahr Medical, Merck, Mirati Therapeutics, Nilogen, Novartis, Champions Oncology, BMS. Consulting fees: AstraZeneca, Hengrui Therapeutics, Mirati Therapeutics, Novartis, Novocure, Regeneron, Sanofi, and Takeda Oncology. Payment or honoraria for lectures, presentations, speakers, bureaus, manuscript writing, or educational events: AstraZeneca, MJH Life Sciences, Novartis, Regeneron, Sanofi, and Takeda. A.S.W. has performed consulting work for MJH Life Sciences and received speaking fees from The Binaytara Foundation and Janssen. L.M.: Travel support: BMS. J.B.: grants for consultancies/advisory boards: BMS, Roche, AstraZeneca. Speaker fees: AstraZeneca, Lilly, Johnson and Johnson. Travel support: Roche, AstraZeneca, MSD, Johnson and Johnson. Research funding (to institution): SEOM. C.G.: grants for consultancies/advisory boards: MSD, BMS, Oncowissen, AstraZeneca, REGENERON, Roche. Speaker fees: AstraZeneca, Boehringer Ingelheim, Chugai, Pierre-Fabre, MSD, Sanofi/REGENERON. Writing/Editorial activity: BMS, MSD. Travel support: Sanofi/REGENERON, MSD. Research fundings (to institution): BMBF/Deutsche Krebshilfe/Deutsche Forschungsgemeinschaft. D.O.: Honorarium: Chugai. Research funding (to institution): Merck, BMS, Palobiofarma, Genentech, AbbVie, Nuvalent, Onc.AI. J.K.H. received consulting honorarium from Jackson Laboratory for Genomic Medicine and ARUP. H.B.: Research Support (Clinical Trials): BMS, Lilly, Amgen; Advisory Board/Consultant: BMS, Lilly, Genentech, Pfizer, Merck, EMD Serono, Boehringer Ingelheim, AstraZeneca, Novartis, Genmab, Regeneron, BioNTech, Amgen, Axiom, PharmaMar, Takeda, Mirati, Daiichi, Guardant, Natera, Oncocyte, Beigene, iTEO, Jazz, Janssen, Puma, BerGenBio, Bayer, Iobiotech, Grid Therapeutics, RAPT; Data and Safety Monitoring Board: University of Pennsylvania: CAR T Program, Takeda, Incyte, Novartis, Springworks; Scientific Advisory Board: Sonnetbio (Stock Options); Inspirna (formerly Rgenix, Stock Options); Nucleai (stock options); Honoraria: Amgen, Pfizer, Daiichi, Regeneron; Travel: Amgen, BMS, Merck, Lilly, EMD Serono, Genentech, Regeneron, Mirati. M.D.: Advisory boards; Sanofi/Genzyme, Regeneron, Janssen, AstraZeneca, Gilead, Bristol Myer Squibb, Catalyst Pharmaceuticals, Novocure, Guardant Consulting: AbbVie, Janssen, Gilead, Daiichi Sankyo, Bristol Myer Squibb Research: Merck, Genentech, CellSight, Novartis, Varian. A.E.: Employee of Caris Life Sciences. J.J.L. has served as a compensated consultant for Genentech, C4 Therapeutics, Blueprint Medicines, Nuvalent, Bayer, Elevation Oncology, Novartis, Mirati Therapeutics, AnHeart Therapeutics, Takeda, CLaiM Therapeutics, Ellipses, Hyku BioSciences, AstraZeneca, Bristol Myers Squibb, Daiichi Sankyo, Yuhan, Merus, Regeneron, Pfizer, Nuvation Bio, and Turning Point Therapeutics; has received institutional research funds from Hengrui Therapeutics, Turning Point Therapeutics, Neon Therapeutics, Relay Therapeutics, Bayer, Elevation Oncology, Roche, Linnaeus Therapeutics, Nuvalent, and Novartis; and travel support from Pfizer and Merus. C.K.: Research funding (to institution): AstraZeneca, Novartis, Regeneron, Janssen, Genentech, Lyell, Daiichi Sankyo, Gilead, Macrogenics, Boehringer Ingelheim, Black Diamond Therapeutics. Consulting fees: Arcus, AstraZeneca, Daiichi Sankyo, Eisai, Regeneron, Sanofi, Takeda, J&J, Pinetree, Boehringer Ingelheim, Gencurix. M.N. is on the advisory board for AstraZeneca, Daiichi Sankyo, Takeda, Novartis, EMD Serono, Janssen, Pfizer, Eli Lilly and Company, Bayer, Regeneron, BMS and Genentech; consultant for Caris Life Sciences (virtual tumor board); speaker for Blueprint Medicines, Janssen, Mirati and Takeda; and reports travel support from AnHeart Therapeutics. Reports stock/stock options from MBrace Therapeutics. T.U.M. currently or has previously served on Advisory and/or Data Safety Monitoring Boards for Rockefeller University, Regeneron, AbbVie, Merck, EMD Serono, Storm, Geneos, Bristol-Meyers Squibb, Boehringer Ingelheim, Atara, AstraZeneca, Genentech, Celldex, Chimeric, DrenBio, Glenmark, Simcere, Arrowhead, Surface/Coherus, G1 Therapeutics, NGMbio, DBV Technologies, Arcus, Fate, Ono, Storm, Replimmune, Larkspur, Avammune, and Astellas, and has research grants from the National Institutes of Health (NCI), the Cancer Research Institute, Regeneron, Genentech, Bristol Myers Squibb, Merck, and Boehringer Ingelheim. A.R.N. reports: Funding to Institution for Trials he is PI on: Loxo@Lilly, Surface Oncology, ADC Therapeutics, IGM Biosciences, EMD Serono, Aravive, Nikang Therapeutics, Inspirna, Exelexis, Revolution Medicine, Jacobio, Pionyr, Jazz Pharmaceuticals, NGM Biopharmaceuticals, Immunocore, Phanes Therapeutics, Kymera Therapeutics, Dren Bio, Daichi; Consultant Editor Compensation: JCO Precision Oncology; Travel Compensation from: SITC/ AACR/ Conquer Cancer Foundation/BinayTara Foundation and Foundation Med/ Caris Life Sciences/ ASCO; Advisory Board: Foundation Med, Astellas, NGM biosciences, Natera, Regeneron; Honoraria: BinayTara Foundation, Foundation Med, Medlive; Grant Support: SOWG Hope Foundation. The remaining authors declare no competing interests.
Figures

References
-
- Travis, W. D. et al. The 2015 World Health Organization Classification of Lung Tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J. Thorac. Oncol.10, 1243–1260 (2015). - PubMed
-
- Jones, M. H. et al. Two prognostically significant subtypes of high-grade lung neuroendocrine tumours independent of small-cell and large-cell neuroendocrine carcinomas identified by gene expression profiles. Lancet363, 775–781 (2004). - PubMed
-
- Bari, M. F. et al. BAI3, CDX2 and VIL1: a panel of three antibodies to distinguish small cell from large cell neuroendocrine lung carcinomas. Histopathology64, 547–556 (2014). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
