

A presentation of posterior reversible encephalopathy syndrome after heart transplantation: a case report and review of literature
- PMID: 40830496
- PMCID: PMC12362904
- DOI: 10.1186/s13256-025-05498-3
A presentation of posterior reversible encephalopathy syndrome after heart transplantation: a case report and review of literature
Abstract
Background: Posterior reversible encephalopathy syndrome is a rare disorder encompassing multiple neurological symptoms usually corroborated by specific neuro magnetic resonance imaging features. Posterior reversible encephalopathy syndrome may be triggered by multiple clinical situations such as blood pressure fluctuations, ischemic stroke, inflammatory and autoimmune disorders, renal failure, pre-eclampsia and eclampsia, hematopoietic stem cell transplantation, cytotoxic drugs, calcineurin inhibitors (cyclosporine A), and other immunosuppressants, as well as a wide range of surgical procedures (mainly cranial and solid organ transplantation). Although rare after cardiac transplantation, posterior reversible encephalopathy syndrome remains a major adverse event among feared complications promoted by use of immunosuppressive drugs. Clinical symptomatology, imaging features, and evolution of posterior reversible encephalopathy syndrome as well therapeutic strategy and identification of contributing factors will be discussed on the basis of our experience and data from literature review.
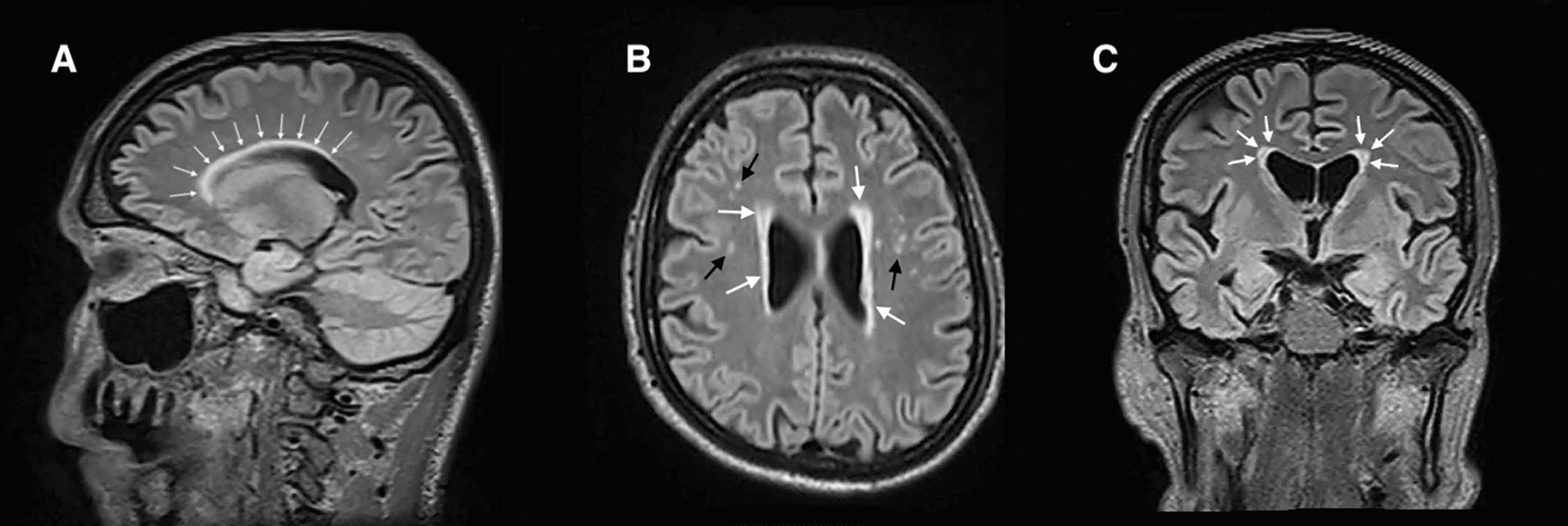
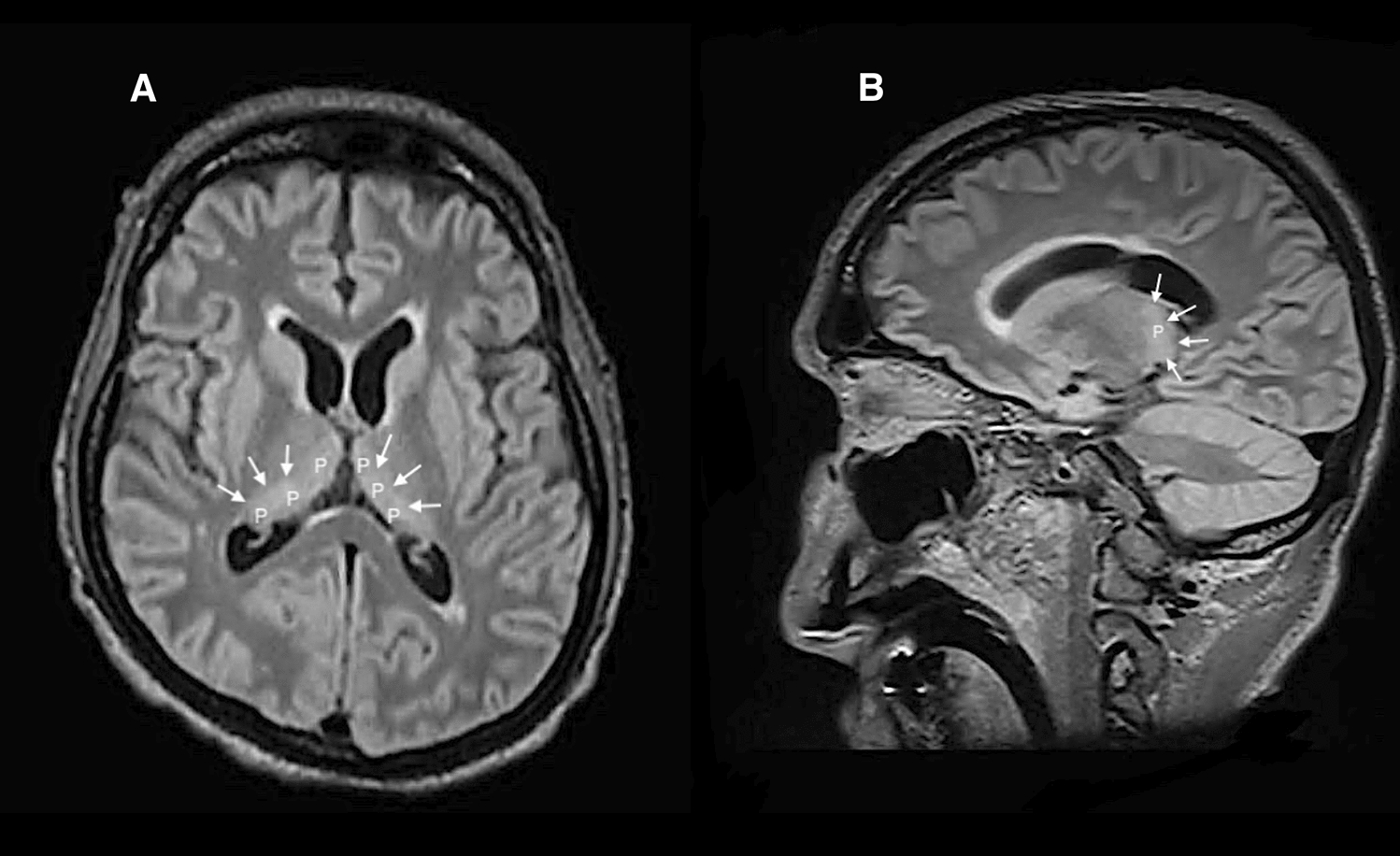
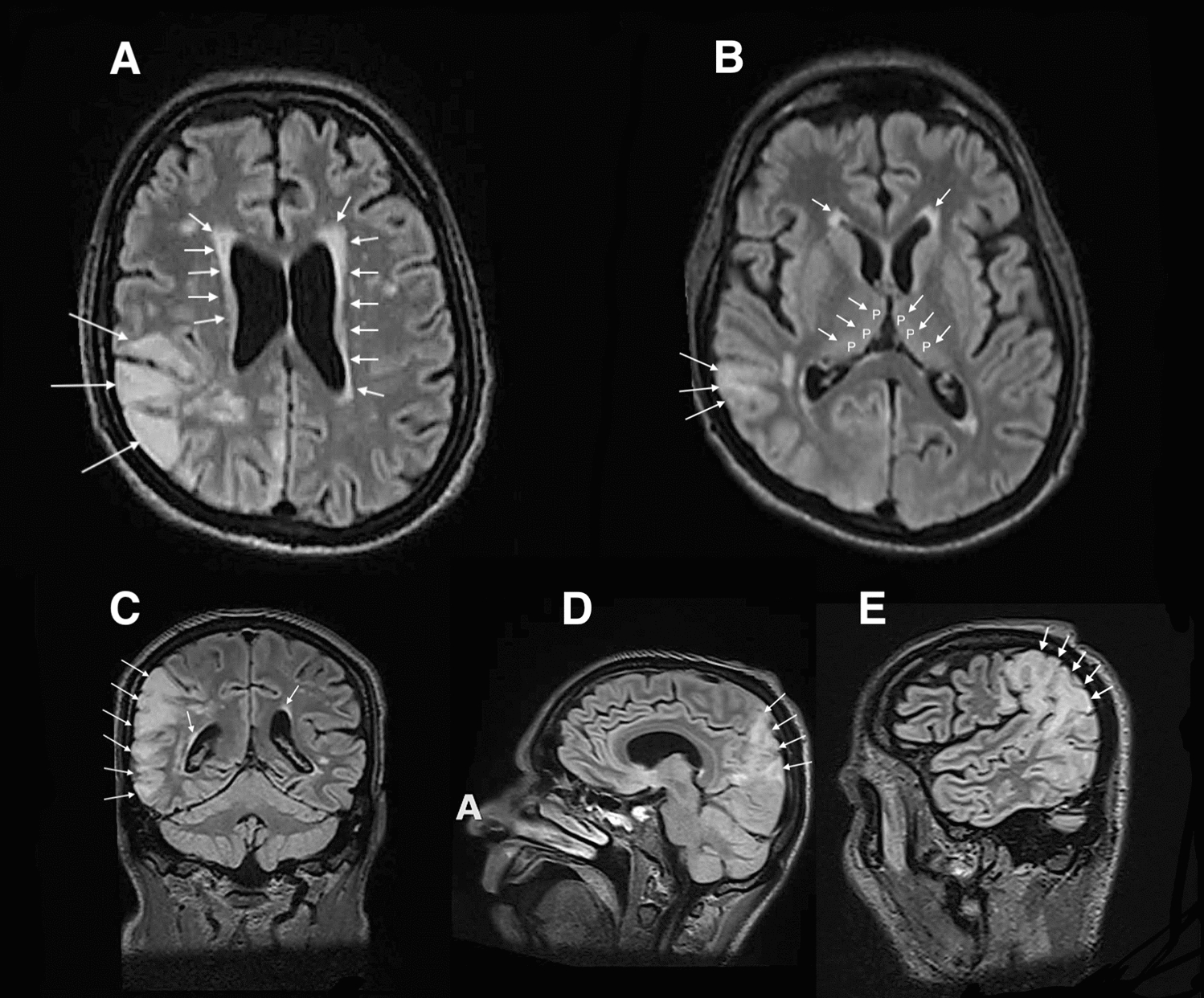
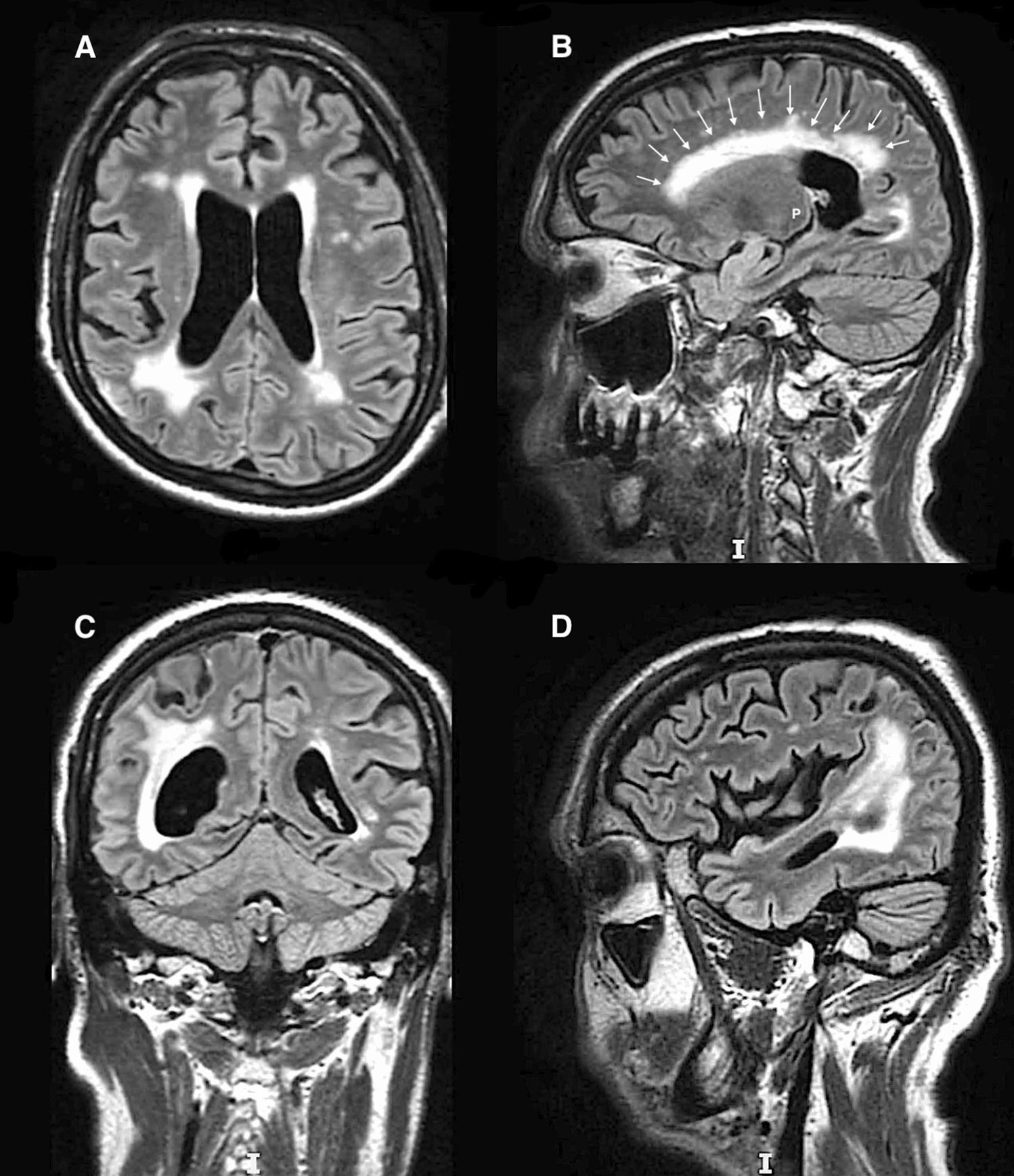
Case presentation: We report the case of a 59-year-old white male patient who was diagnosed with posterior reversible encephalopathy syndrome 3 months after cardiac transplantation. Neurologic complications gradually worsened within weeks after transplantation from an immediate postoperative paraparesis to seizures and coma requiring specific management in the intensive care unit. Initial brain computed tomography and magnetic resonance imaging were not contributive. Ultimately, magnetic resonance imaging characteristics of posterior reversible encephalopathy syndrome gradually appeared 10 weeks after transplantation and were concomitant with epileptic seizures, coma, and occurrence of Shiga toxin-producing Escherichia coli-hemolytic-uremic syndrome in a context of blood pressure variations and administration of cyclosporine A.
Conclusion: This case highlighted the necessity for clinicians to be familiar with posterior reversible encephalopathy syndrome to prevent misdiagnosis and optimize neurological outcomes. In addition, it emphasized the underlying non-dose-dependent neurotoxicity of cyclosporine A.
Keywords: Calcineurin inhibitors; Cerebral MRI; Cyclosporine A; Hemolytic uremic syndrome; Posterior reversible encephalopathy syndrome; Shiga toxin-producing Escherichia coli; Solid organ transplantation; Status epilepticus; Tacrolimus.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The privacy of the patient was considered, and the manuscript does not display any identifying information. Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Competing interests: The authors declare that they have no competing interests.
Figures

References
-
- Hinchey J, Chaves C, Appignani B, Breen J, Pao L, Wang A, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med. 1996;334(8):494–500. 10.1056/NEJM199602223340803. - PubMed
-
- Marra A, Vargas M, Striano P, Del Guercio L, Buonanno P, Servillo G. Posterior reversible encephalopathy syndrome: the endothelial hypotheses. Med Hypotheses. 2014;82(5):619–22. 10.1016/j.mehy.2014.02.022. - PubMed
-
- Ho ML, Rojas R, Eisenberg RL. Cerebral edema. AJR Am J Roentgenol. 2012;199(3):W258–73. 10.2214/AJR.11.8081. - PubMed
-
- Doelken M, Lanz S, Rennert J, Alibek S, Richter G, Doerfler A. Differentiation of cytotoxic and vasogenic edema in a patient with reversible posterior leukoencephalopathy syndrome using diffusion-weighted MRI. Diagn Interv Radiol. 2007;13(3):125–8. - PubMed
-
- Vanacker P, Matias G, Hagmann P, Michel P. Cerebral hypoperfusion in posterior reversible encephalopathy syndrome is different from transient ischemic attack on CT perfusion. J Neuroimaging. 2015;25(4):643–6. 10.1111/jon.12158. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
