

Eye movement features for assisting differentiation between posterior circulation infarction and vestibular neuritis in patients of acute vestibular syndrome
- PMID: 40830990
- PMCID: PMC12366142
- DOI: 10.1186/s40001-025-03046-9
Eye movement features for assisting differentiation between posterior circulation infarction and vestibular neuritis in patients of acute vestibular syndrome
Abstract
Introduction: A significant portion of patients with acute vestibular syndrome (AVS) due to posterior circulation infarction (PCI) is free of non-vestibular signs. A differential diagnosis of this form from that due to vestibular neuritis (VN) can be challenging. We herein aimed to understand whether quantitative eye movement signature could be used to assist such a diagnosis.
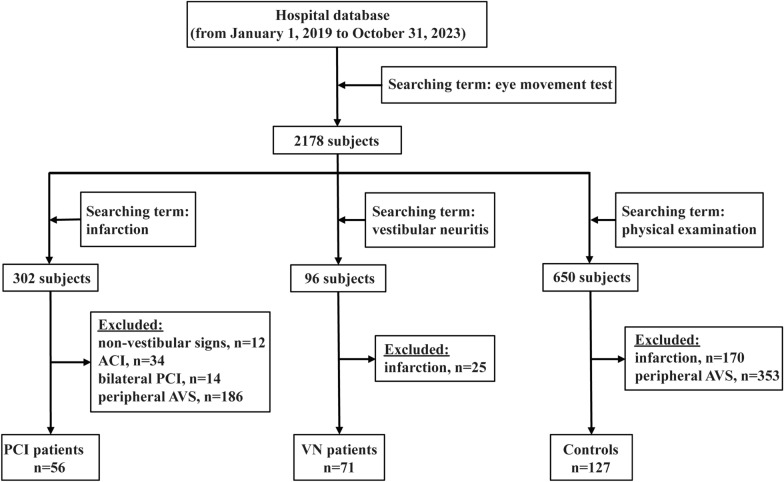
Methods: A total of 56 patients with AVS due to PCI free of non-vestibular signs, 71 patients with AVS due to VN, and 127 controls were selected retrospectively into the study from our hospital database. Demographic, clinical data, and videooculography results were extracted.
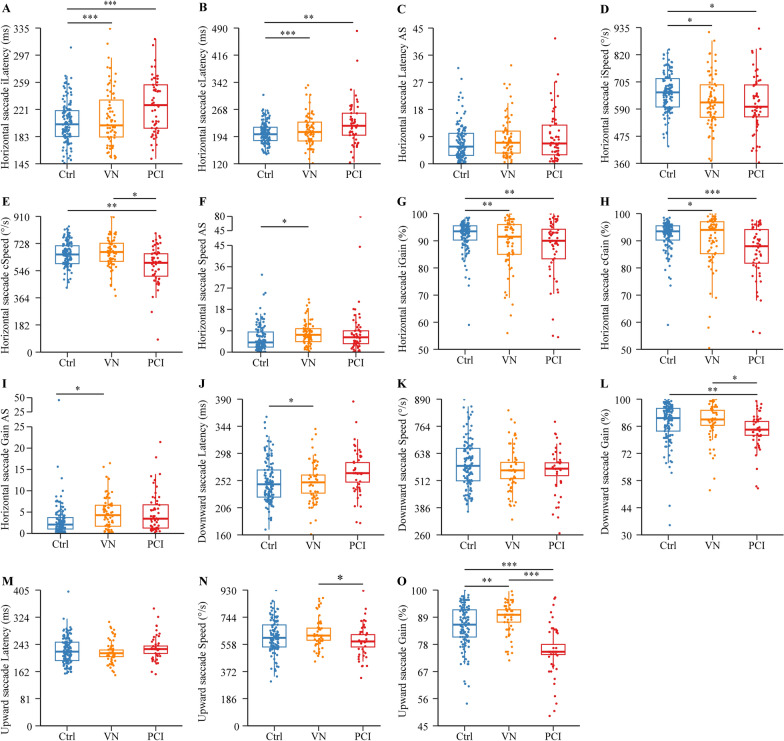
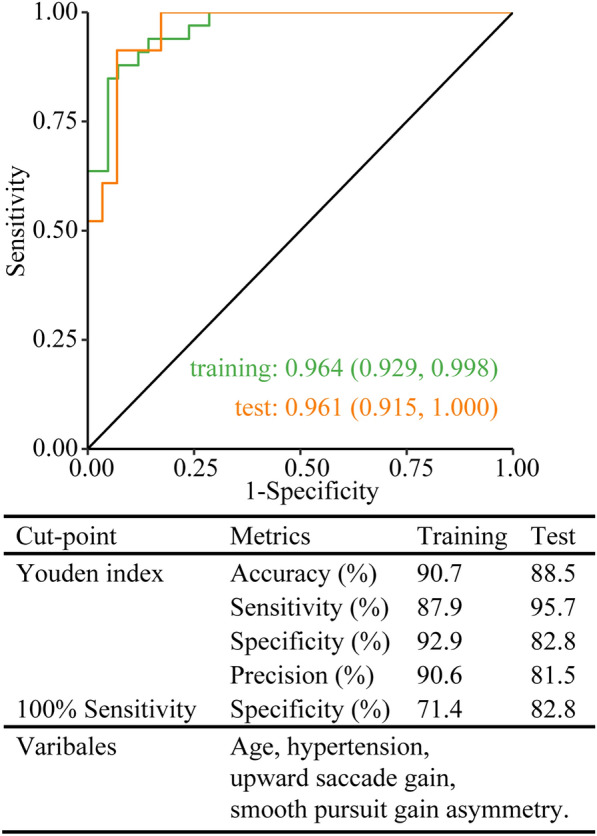
Results: Patients with PCI or VN differed from controls in most eye movement metrics. Patients with PCI also differed from those with VN in multiple metrics, including contralesional speed of horizontal saccade, gain of downward saccade, speed and gain of upward saccade, contralesional gain and gain asymmetry of smooth pursuit, and ipsilesional gain of optokinetic nystagmus. A detection model, built on the basis of age, hypertension, gain of upward saccade, and gain asymmetry of smooth pursuit, distinguished PCI from VN with area under the curve at 0.964 (0.929, 0.998) and 0.961 (0.915, 1.000) in the training and test sessions, respectively.
Conclusion: We demonstrate that eye movements are differentially impaired in patients with PCI free of non-vestibular signs and those with VN. The detection model built on smooth pursuit gain asymmetry and upward saccade gain may assist the differentiation between PCI and VN in AVS patients by trained clinicians.
Keywords: Diagnosis modeling; Peripheral origin; Retrospective analysis; Side of lesion; Stroke.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the ethics committee of Wenzhou Central Hospital (approval No. L2023-04–052). All data used in this study were acquired from the hospital database and were de-identified appropriately; thus, no informed consent from subjects was obtained. Competing interests: The authors declare no competing interests.
Figures

References
-
- Hotson JR, Baloh RW. Acute vestibular syndrome. N Engl J Med. 1998;339(10):680–5. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
