

To elucidate the effect of Ruanjian Qingmai granules on arteriosclerosis obliterans from the perspective of cholesterol efflux
- PMID: 40832101
- PMCID: PMC12358959
- DOI: 10.3389/fmed.2025.1510927
To elucidate the effect of Ruanjian Qingmai granules on arteriosclerosis obliterans from the perspective of cholesterol efflux
Abstract
Aim of the study: To investigate the effect of Ruanjian Qingmai granules (RJQM) on arteriosclerotic obliterans (ASO) and identify its potential bioactive components.
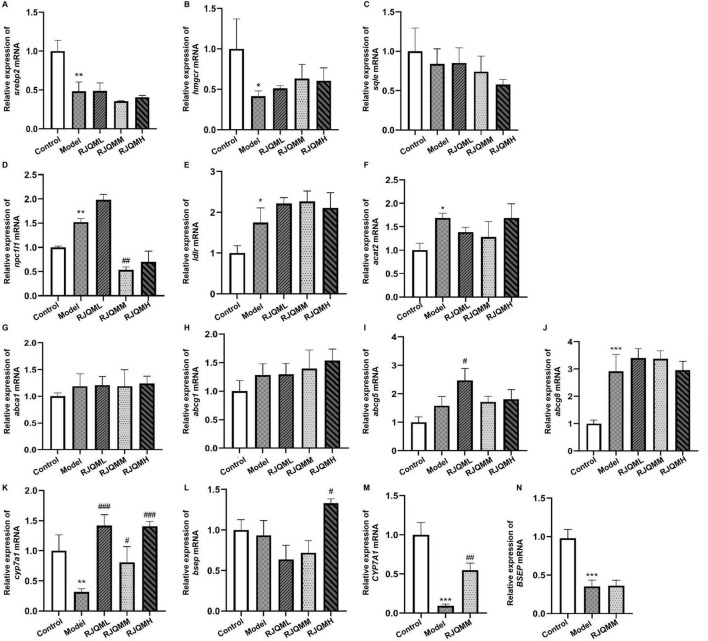
Materials and methods: Separate zebrafish atherosclerosis models and cellular lipid metabolism disorder models were established, and RJQM was administered at different concentrations for intervention. The lipid deposition was examined by using Nile Red staining. The expression levels of cholesterol metabolism-related genes were determined by using quantitative real-time PCR (qRT-PCR). The CYP7A1 inhibitor was utilized to elucidate the target of RJQM. Through network pharmacology and serum pharmacochemistry approaches, potential bioactive components were systematically identified and subsequently validated through experimental assays.
Results: Ruanjian Qingmai granules significantly decreased lipid deposition and significantly increased the expression of CYP7A1 mRNA in both zebrafish and HepaRG cells. And this effect was attenuated by CYP7A1 inhibitors. Serum pharmacochemistry and network pharmacological analysis indicated that kaempferol and isorhamnetin were potential bioactive components in RJQM for the treatment of ASO. Both components could significantly reduce lipid deposition in zebrafish and HepaRG cells, and this effect was also diminished by CYP7A1 inhibitors. Molecular docking also confirmed that CYP7A1 might be the target of kaempferol and isorhamnetin, and qRT-PCR results also verified that both components could significantly up-regulate the mRNA expression level of CYP7A1.
Conclusion: Ruanjian Qingmai granules exerts a therapeutic effect on ASO by up-regulating the expression level of CYP7A1 mRNA, thereby reprogramming lipid metabolism. Kaempferol and isorhamnetin are likely the main active components of RJQM in lipid metabolic reprogramming.
Keywords: CYP7A1; Ruanjian Qingmai granules; arteriosclerosis obliterans; lipid reprogramming; potential bioactive components.
Copyright © 2025 Jia, Hong, Jiang, Ma, Liu, Xu, Chen, Xie, Ge, Cao, Yan and Cao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






References
-
- Gerhard-Herman M, Gornik H, Barrett C, Barshes N, Corriere M, Drachman D, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: A report of the american college of cardiology/American heart association task force on clinical practice guidelines. Circulation. (2017) 135:e726–79. 10.1161/CIR.0000000000000471 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources