

Gastrointestinal stromal tumor with secondary thrombocytosis: a case report of a high-risk patient
- PMID: 40837560
- PMCID: PMC12361118
- DOI: 10.3389/fmed.2025.1605819
Gastrointestinal stromal tumor with secondary thrombocytosis: a case report of a high-risk patient
Abstract
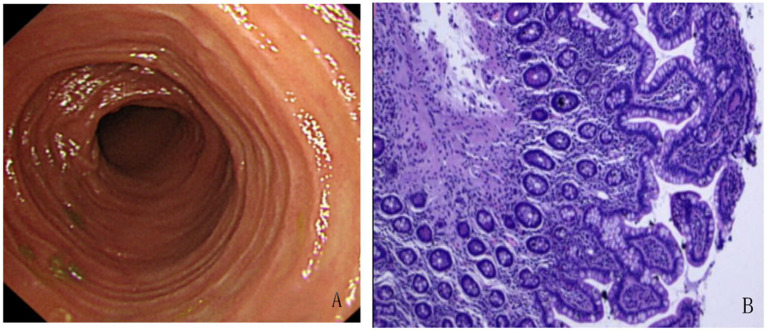
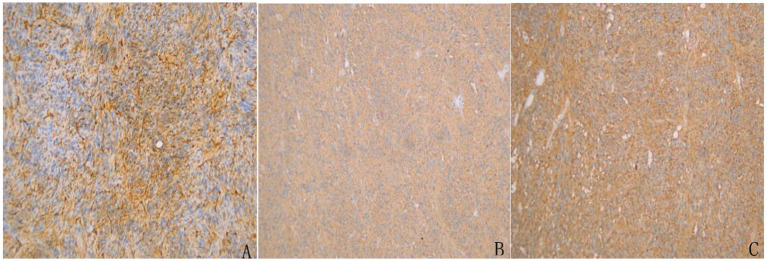
Gastrointestinal stromal tumor (GIST) with secondary thrombocytosis is a rare clinical case, exhibiting specificity in clinical diagnosis and treatment. We report a case of GIST with secondary thrombocythemia to raise clinicians' attention to this disease. On October 11, 2024, a 58-year-old male patient was admitted to the hospital due to "intermittent right lower abdominal pain with increased bowel movements for more than 1 month." The patient had no prior history of tumors, chronic inflammatory diseases, hematologic disorders or family history of genetic disorders. MRI-enhanced scans of the small intestine highly indicated a lymphoma of intestinal origin. Small bowel endoscopy and pathological biopsy revealed mild chronic inflammation of the intestinal mucosa, with intact villous architecture, no plasmacytosis, granulomas, or vasculitis, and no indication of GIST. Laboratory tests showed platelet count of 909 × 109/L, white blood cell count of 11.86 × 109/L, neutrophil ratio of 75.10%, lymphocyte ratio of 15.30% and hemoglobin 101 g/L. Bone marrow biopsy microscopically showed a normal number of megakaryocytes without abnormal aggregation and no myelofibrosis, suggesting there was no obvious hematologic malignancy and the thrombocytosis may have been secondary. The patient underwent partial resection of the small intestine and resection of mesenteric lesions on October 18, 2024. The intraoperative frozen section suggested a stromal tumor. The postoperative pathological biopsy suggested a GIST and genetic testing showed a mutation in the c-KIT gene (Exon 13). Postoperatively, the patient was treated with oral imatinib mesylate (400 mg/d) as adjunctive therapy. Three months after surgery, imaging showed no recurrence, platelet decreased and returned to normal levels.
Keywords: Exon 13; c-KIT; case report; gastrointestinal stromal tumor; secondary thrombocythemia.
Copyright © 2025 Li, Liu, Guo, Wang, Han and Mao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Severe Relapsing Hailey-Hailey Disease Displaying a Durable Complete Response to Hydroxyurea.Acta Dermatovenerol Croat. 2024 Nov;32(3):168-169. Acta Dermatovenerol Croat. 2024. PMID: 40654217
-
Imatinib for the treatment of patients with unresectable and/or metastatic gastrointestinal stromal tumours: systematic review and economic evaluation.Health Technol Assess. 2005 Jul;9(25):1-142. doi: 10.3310/hta9250. Health Technol Assess. 2005. PMID: 15985189
-
Prophylactic platelet transfusion for prevention of bleeding in patients with haematological disorders after chemotherapy and stem cell transplantation.Cochrane Database Syst Rev. 2012 May 16;2012(5):CD004269. doi: 10.1002/14651858.CD004269.pub3. Cochrane Database Syst Rev. 2012. PMID: 22592695 Free PMC article.
-
Sympathetic nerve blocks for persistent pain in adults with inoperable abdominopelvic cancer.Cochrane Database Syst Rev. 2024 Jun 6;6(6):CD015229. doi: 10.1002/14651858.CD015229.pub2. Cochrane Database Syst Rev. 2024. PMID: 38842054 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources