

Ganglion cell layer changes following the idiopathic macular hole surgery using inverted limiting membrane flap technique
- PMID: 40841609
- PMCID: PMC12372387
- DOI: 10.1186/s12886-025-04317-z
Ganglion cell layer changes following the idiopathic macular hole surgery using inverted limiting membrane flap technique
Abstract
Purpose: The purpose of this study is to compare the ganglion cell layer changes following temporal inverted internal limiting membrane flap (i-ILMF) surgery for idiopathic macular hole (IMH).
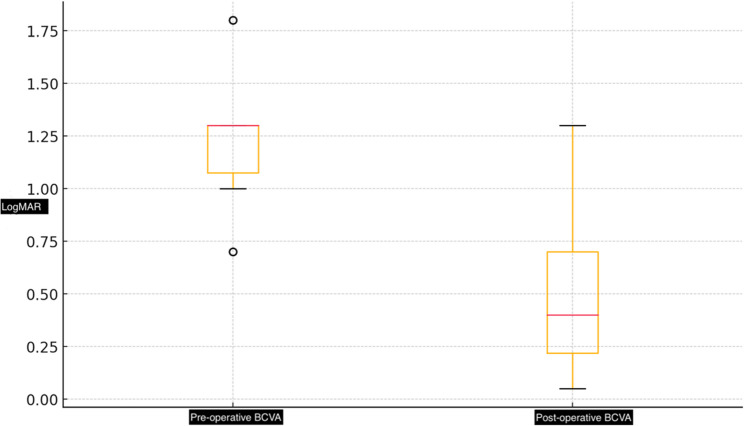
Methods: This retrospective study included 50 eyes that underwent vitrectomy with a 2.5-disc-diameter temporal inverted internal limiting membrane flap (i-ILMF) technique. Demographic, functional, and anatomical data were collected before and after the surgery. The best corrected visual acuity (BCVA) and optical coherence tomography (OCT) findings such as ganglion cell layer -inner plexiform layer (GCL-IPL) thickness and hole related parameters/indexes were compared in the preoperative period and 6th month after surgery.
Results: The average age of the patients was 68.8 ± 10.31 years, and the average duration of visual loss was 10.95 ± 6.54 months. The average GCL-IPL thickness increased significantly from 57.98 ± 21.43 μm to 68.74 ± 13.62 μm at 6 months after surgery (p < 0.001). The nasal GCL-IPL thickness was significantly increased from 56.94 ± 24.18 μm to 73.10 ± 15.39 μm after 6 months after surgery (p < 0.001).
Conclusion: The temporal i-ILMF technique not only leads to high anatomical success and visual improvement but also results in a significant increase in GCL-IPL thickness postoperatively, suggesting a unique structural response to this method.
Keywords: Ganglion cell layer; Idiopathic macular hole; Temporal inverted internal limiting membrane flap technique.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All patients provided informed consent in accordance with the guidelines approved by the ethics committee. The study received ethics committee approval from Ankara City Hospital (E1/1750/2021). All procedures performed in studies involving human participants were in accordance with the Helsinki declaration and its later amendments or comparable ethical standards. Competing interests: The authors declare no competing interests.
Figures





References
-
- Brooks HL. Macular hole surgery with and without internal limiting membrane peeling. Ophthalmology. 2000;107:1939–48. - PubMed
-
- Baba T, Hagiwara A, Sato E, Arai M, Oshitari T, Yamamoto S. Comparison of vitrectomy with brilliant blue G or indocyanine green on retinal microstructure and function of eyes with macular hole. Ophthalmology. 2012;119:2609–15. - PubMed
-
- Imai M, Iijima H, Gotoh T, Tsukahara S. Optical coherence tomography of successfully repaired idiopathic macular holes. Am J Ophthalmol. 1999;128:621–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
