

Harm reduction measures in a recreational gym user with anabolic androgenic steroid dependence: a case report in the context of current best clinical practice
- PMID: 40841640
- PMCID: PMC12369084
- DOI: 10.1186/s12954-025-01294-w
Harm reduction measures in a recreational gym user with anabolic androgenic steroid dependence: a case report in the context of current best clinical practice
Abstract
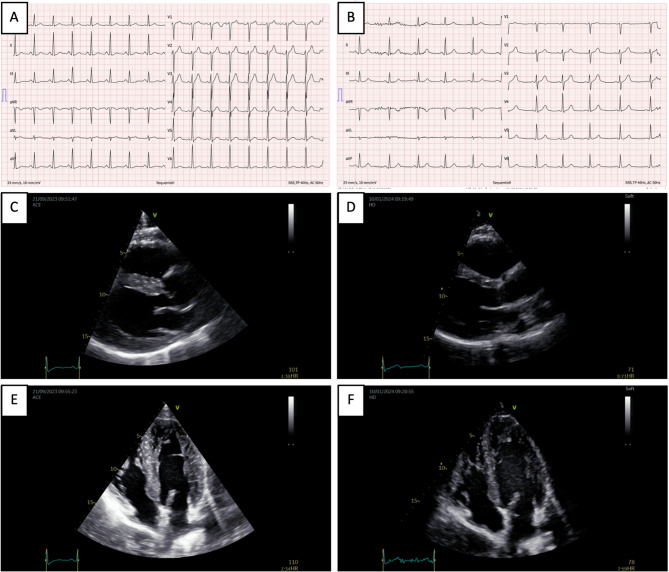
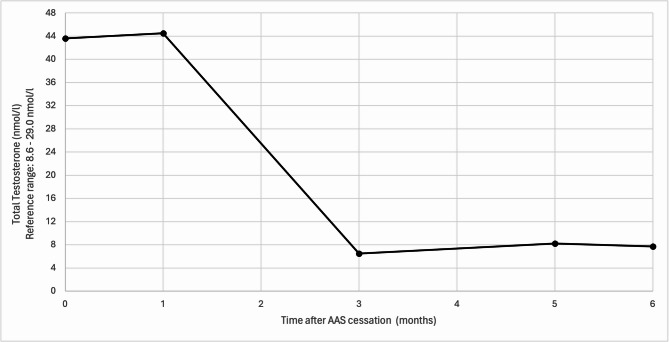
Introduction: The non-medical use of androgens among recreational gym users has become a global substance use concern. Complications from use particularly appear to affect the cardiovascular system, including the development of cardiovascular events, as well as anabolic steroid-induced cardiomyopathy (ASIC). Furthermore, the development of substance dependence with a specific withdrawal syndrome appears to be common and is contributed by the development of endocrine dysfunction related to anabolic steroid-induced hypogonadism. A 38-year-old male law enforcement officer and recreational bodybuilder presented with multiple health complaints following years of supraphysiologic androgen use and polypharmacy. Key symptoms included new-onset subacute dyspnea, dizziness, palpitations, headaches, and recurrent failed attempts at androgen cessation. Clinical findings showed abnormal blood pressure, testicular atrophy, plethoric appearance, and laboratory evidence of progressive polycythemia (hematocrit: 56.9%; normal < 49%), elevated testosterone, and suppressed luteinizing and follicle-stimulating hormones. He was at risk for muscle dysmorphia and met criteria for androgen dependence. Diagnosis confirmed ASIC. Treatment consisted of recurrent bloodletting for polycythemia, guideline-based cardiac management, and a structured endocrine regimen (tapered transdermal testosterone, oral Tamoxifen, subcutaneous human chorionic gonadotropin) to support androgen discontinuation and hormonal recovery. At 4 months, ASIC had normalized, and he was asymptomatic. However, after 6 months, he developed laboratory-confirmed idiopathic primary hypogonadism and began guideline-directed testosterone replacement. Despite more than a year of abstinence from non-medical androgen use and normalization of cardiac function, the patient died from a cardiovascular event, highlighting the possibly persistent risks of prior androgen use.
Conclusion: Non-medical androgen use is a growing global issue among recreational gym-goers. The intersection of severe health risks and substance dependence highlights the urgent need for an integrated, medical and harm-reduction approach-ideally delivered in specialized primary care settings. Early detection of cardiovascular risk factors is crucial for mitigating the often-overlooked yet potentially reversible complications. A reassessment of legal and clinical measures is warranted to optimize harm reduction and provision of care. Despite best practices and a year of abstinence from non-medical androgen use, the patient's fatal outcome underscores the critical need for further research, heightened awareness, and more robust prevention and harm reduction strategies for those affected by non-medical androgen use.
Keywords: Addiction; Anabolic androgenic steroids; Cardiomyopathy; Case report; Hypogonadism; Polycythemia; Substance use disorder.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This case report does not require ethical approval. Consent for publication: The patient has read the final manuscript for initial submission and provided informed consent for publication. Competing interests: The authors have no relevant financial or non-financial interests to disclose. We can report that there is no conflict of interest.
Figures
References
-
- Ip EJ, Lu DH, Barnett MJ, Tenerowicz MJ, Vo JC, Perry PJ. Psychological and physical impact of anabolic-androgenic steroid dependence. Pharmacotherapy. 2012;32(10):910–9. - PubMed
-
- Kanayama G, Pope HG. History and epidemiology of anabolic androgens in athletes and non-athletes. Mol Cell Endocrinol. 2018;464:4–13. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
