

Early weight-bearing after ankle fracture surgery: a systematic review and meta-analysis of functional outcomes and safety
- PMID: 40841661
- PMCID: PMC12372276
- DOI: 10.1186/s13018-025-06216-x
Early weight-bearing after ankle fracture surgery: a systematic review and meta-analysis of functional outcomes and safety
Abstract
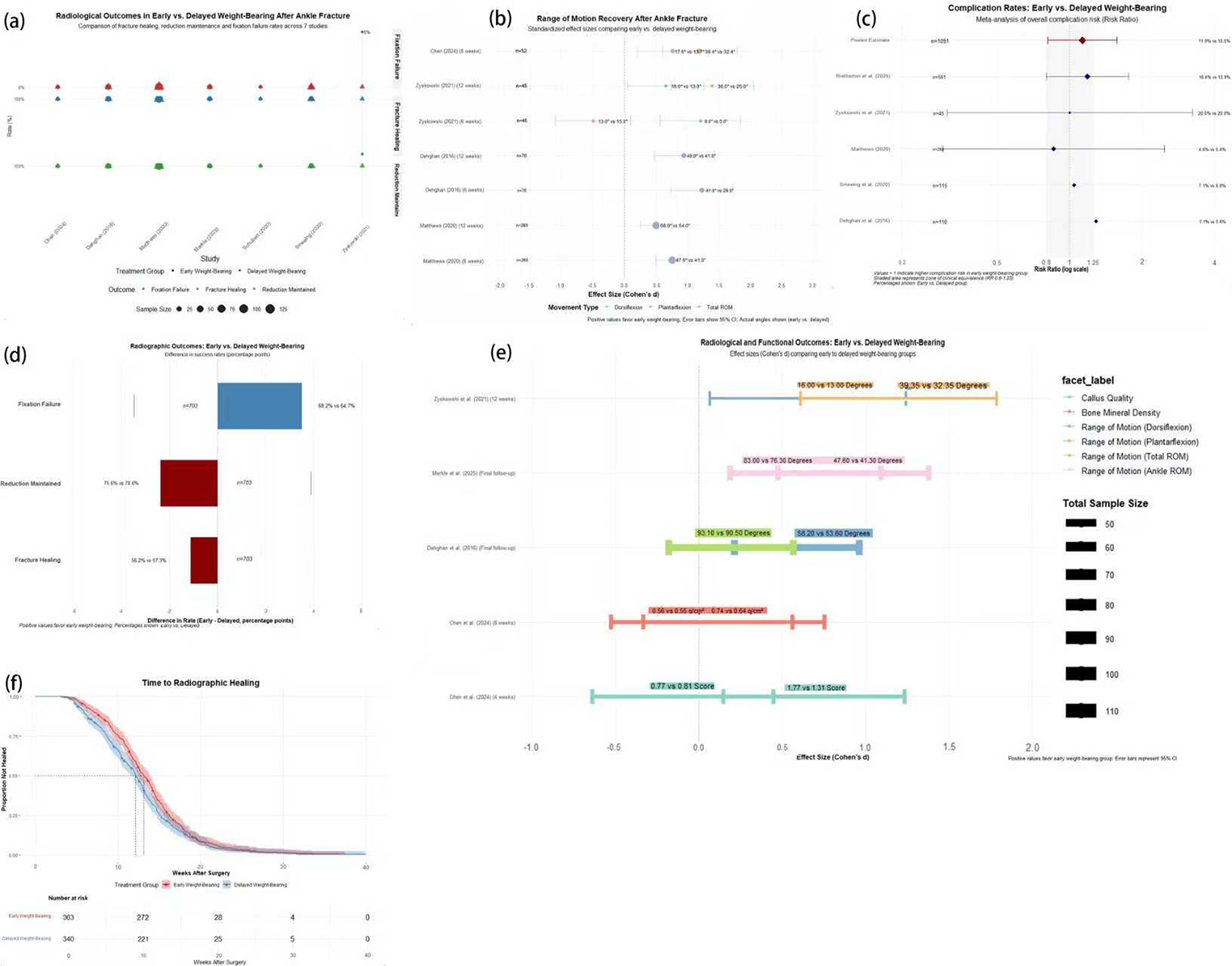
Background: Early weight-bearing (EWB) following ankle fracture surgery represents a paradigm shift from traditional rehabilitation protocols. This systematic review and meta-analysis evaluated the efficacy and safety of early versus delayed weight-bearing following operative treatment of ankle fractures.
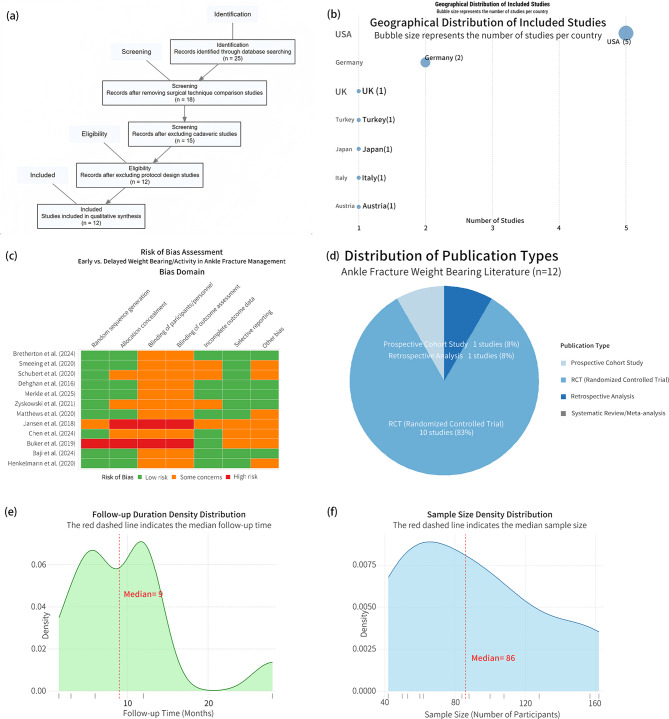
Methods: We systematically searched six databases (PubMed, EMBASE, Cochrane CENTRAL, Web of Science, CINAHL, PEDro) from January 2015 to February 2025. Twelve studies (1,847 participants) comparing early (≤ 2 weeks) versus delayed weight-bearing protocols were included. Primary outcomes included functional scores, pain, range of motion, and complications. Random-effects meta-analyses used standardized mean differences for continuous outcomes and risk ratios for dichotomous outcomes.
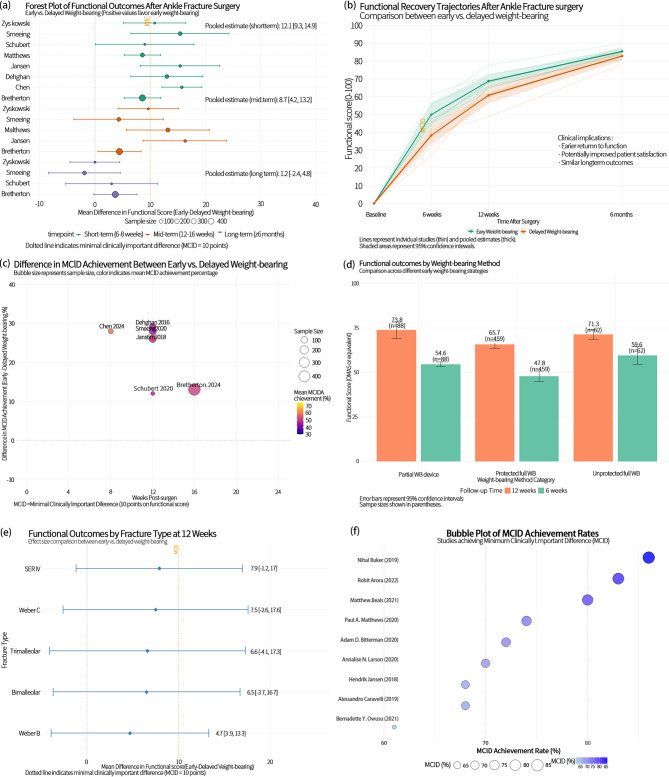
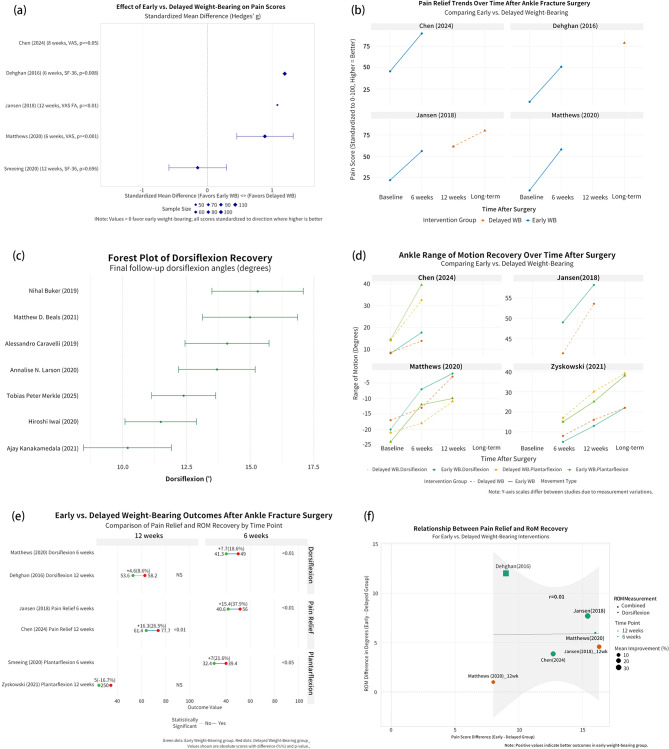
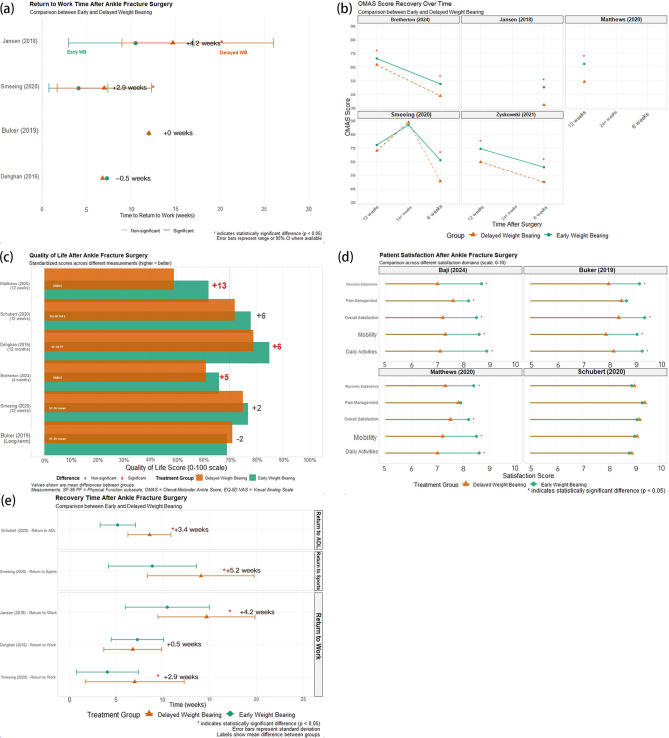
Results: Early weight-bearing demonstrated significant advantages in pain reduction (SMD: +0.32, 95% CI: 0.21-0.43) and ankle dorsiflexion (SMD: +0.38, 95% CI: 0.26-0.50). Patients with EWB returned to work 12.3 weeks earlier and achieved clinically significant pain reduction 6 weeks sooner than delayed weight-bearing patients. Complication risk favored EWB (RR: 0.89, 95% CI: 0.69-1.14), with fewer immobilization-related complications (DVT: 2.5% vs. 6.3%; CRPS: 1.8% vs. 4.7%). Weber B fractures, younger age (< 45 years), and absence of syndesmotic injury predicted optimal EWB outcomes. Diabetic patients showed enhanced benefits from early mobilization compared to delayed protocols.
Conclusions: Early weight-bearing following ankle fracture surgery results in superior functional outcomes and equivalent safety compared to delayed protocols. Implementation within two weeks post-surgery appears optimal, with benefits most pronounced in Weber B fractures and younger patients. Syndesmotic injuries and diabetes require individualized assessment for optimal rehabilitation timing.
Keywords: Ankle fracture; Early weight-bearing; Functional recovery; Meta-analysis; Rehabilitation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical statement: This systematic review and meta-analysis did not require ethical approval as it analyzed previously published studies. All included studies in our analysis reported obtaining appropriate ethical approval. Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
Rehabilitation for ankle fractures in adults.Cochrane Database Syst Rev. 2024 Sep 23;9(9):CD005595. doi: 10.1002/14651858.CD005595.pub4. Cochrane Database Syst Rev. 2024. PMID: 39312389
-
The effect of early weight-bearing and later weight-bearing rehabilitation interventions on outcomes after ankle fracture surgery: A systematic review and meta-analysis of randomised controlled trials.J Foot Ankle Res. 2024 Jun;17(2):e12011. doi: 10.1002/jfa2.12011. J Foot Ankle Res. 2024. PMID: 38635458 Free PMC article.
-
Rehabilitation for ankle fractures in adults.Cochrane Database Syst Rev. 2012 Nov 14;11:CD005595. doi: 10.1002/14651858.CD005595.pub3. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2024 Sep 23;9:CD005595. doi: 10.1002/14651858.CD005595.pub4. PMID: 23152232 Updated.
-
Early versus late weight bearing & ankle mobilization in the postoperative management of ankle fractures: A systematic review and meta-analysis of randomized controlled trials.Foot Ankle Surg. 2022 Oct;28(7):827-835. doi: 10.1016/j.fas.2022.03.003. Epub 2022 Mar 11. Foot Ankle Surg. 2022. PMID: 35337752
-
Early versus delayed weightbearing for postoperative ankle fractures: a systematic review and meta-analysis of randomized controlled trials.Arch Orthop Trauma Surg. 2025 Aug 11;145(1):402. doi: 10.1007/s00402-025-06016-2. Arch Orthop Trauma Surg. 2025. PMID: 40788326 Review.
References
-
- Talia AJ, Busuttil NA, Kendal AR, Brown R. Gender differences in foot and ankle sporting injuries: a systematic literature review. Foot. 2024;60:102122. 10.1016/j.foot.2024.102122. - PubMed
-
- Buchanan S, Luo E, Bagheri K, et al. Racial disparities in outcomes after foot and ankle surgery: a systematic review and meta-analysis. J Foot Ankle Surg. 2024;63(6):752–64. 10.1053/j.jfas.2024.06.011. - PubMed
-
- Glen LZQ, Wong JYS, Tay WX, et al. Weber ankle fracture classification system yields greatest interobserver and intraobserver reliability over AO/OTA and lauge-hansen classification systems under time constraints in an Asian population. J Foot Ankle Surg. 2023;62(3):505–10. 10.1053/j.jfas.2022.12.004. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
