

Individualized transcranial direct current stimulation combined with foot core exercise improves foot and ankle sensorimotor function and static postural control in individuals with chronic ankle instability
- PMID: 40841683
- PMCID: PMC12369118
- DOI: 10.1186/s12984-025-01721-w
Individualized transcranial direct current stimulation combined with foot core exercise improves foot and ankle sensorimotor function and static postural control in individuals with chronic ankle instability
Abstract
Objective: This study aimed to investigate the effects of four-week individualized transcranial direct current stimulation (tDCS) combined with foot core exercise (FCE) on foot and ankle sensorimotor function and postural control in individuals with chronic ankle instability (CAI).
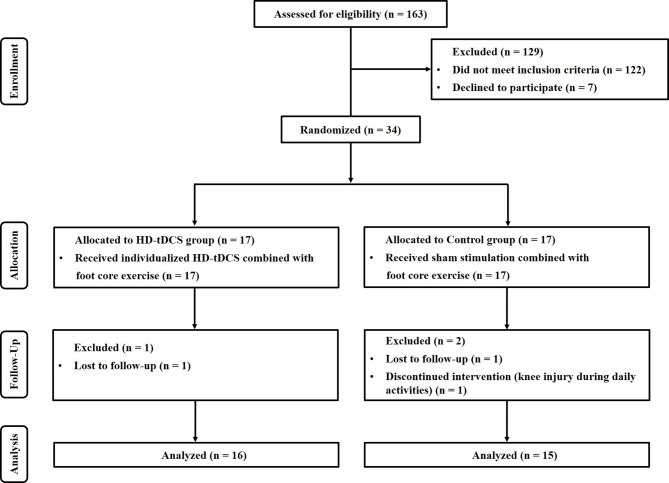
Methods: Thirty-four CAI individuals were randomly assigned to a tDCS combined with FCE group (tDCS group, n = 17) and a sham stimulation combined with FCE group (control group, n = 17). All participants received individualized stimulation combined with FCE and sham stimulation combined with FCE, respectively, three times a week for 20 min per session over four weeks. Ankle strength, joint position sense, and static and dynamic postural control were assessed at baseline and post-intervention.
Results: Compared with the control group and baseline, individualized tDCS combined with FCE significantly increased the relative peak torque of plantarflexion, reduced the absolute error of ankle eversion position sense, and decreased the average sway velocity of the center of pressure during single-leg standing with eyes closed in CAI individuals (p values ranging from < 0.001 to 0.016).
Conclusion: Four weeks of individualized tDCS combined with FCE can effectively improve foot and ankle sensorimotor function and static postural control in CAI individuals.
Keywords: Ankle strength; Chronic ankle instability; Foot core exercise; Individualized transcranial direct current stimulation; Joint position sense; Postural control.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Ethics Committee of the Shanghai University of Sport (No. 102772022RT049). All participants provided written informed consent prior to participation. Consent for publication: All participants in this study received instructions about the experimental procedures and content and provided written informed consent. Competing interests: The authors declare no competing interests.
Figures




References
-
- Waterman BR, Owens BD, Davey S, Zacchilli MA, Belmont PJ. The epidemiology of ankle sprains in the united States. J Bone Joint Surg Am. 2010;92(13):2279–84. - PubMed
-
- Gribble PA, Bleakley CM, Caulfield BM, Docherty CL, Fourchet F, Fong DT, et al. Evidence review for the 2016 international ankle consortium consensus statement on the prevalence, impact and long-term consequences of lateral ankle sprains. Br J Sports Med. 2016;50(24):1496–505. - PubMed
-
- Vuurberg G, Hoorntje A, Wink LM, van der Doelen BFW, van den Bekerom MP, Dekker R, et al. Diagnosis, treatment and prevention of ankle sprains: update of an evidence-based clinical guideline. Br J Sports Med. 2018;52(15):956. - PubMed
-
- Munn J, Sullivan SJ, Schneiders AG. Evidence of sensorimotor deficits in functional ankle instability: a systematic review with meta-analysis. J Sci Med Sport. 2010;13(1):2–12. - PubMed
-
- Holmes A, Delahunt E. Treatment of common deficits associated with chronic ankle instability. Sports Med. 2009;39(3):207–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
