

Giant Pheochromocytoma With Non-classical Symptoms: A Case Report to Expand Clinical Awareness
- PMID: 40842753
- PMCID: PMC12366873
- DOI: 10.7759/cureus.88445
Giant Pheochromocytoma With Non-classical Symptoms: A Case Report to Expand Clinical Awareness
Abstract
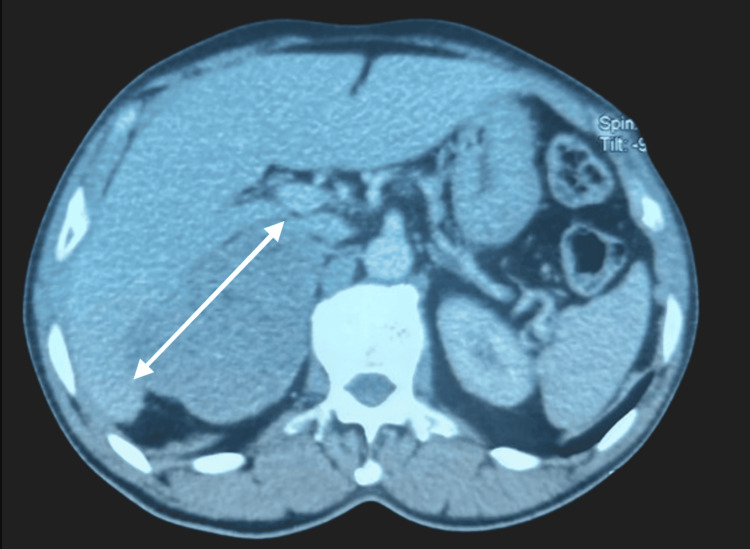
Pheochromocytomas are rare neuroendocrine tumors arising from chromaffin cells of the adrenal medulla or extra-adrenal paraganglia. Their clinical presentation varies widely among individuals and is primarily linked to the biological effects of excessive catecholamine secretion. We report an unusual case of pheochromocytoma presenting as epigastric heaviness. A 65-year-old male with a known history of type 2 diabetes mellitus, treated with metformin, and well-controlled hypertension managed with amlodipine, presented with a complaint of persistent epigastric heaviness in the absence of associated symptoms. Abdominal CT imaging revealed a large, locally infiltrative right adrenal mass measuring 92 x 82 x 80 mm. As part of the etiological work-up, serum potassium and urinary cortisol levels were within normal limits. The diagnosis of pheochromocytoma was established based on significantly elevated urinary metanephrines and normetanephrines, exceeding the normal values by 55-fold and 23-fold, respectively. The evaluation for multiple endocrine neoplasia syndromes was negative. Iodine-123 metaiodobenzylguanidine (¹²³I-MIBG) scintigraphy confirmed the presence of a hyperfixating adrenal mass, consistent with pheochromocytoma. Following adequate preoperative pharmacologic preparation, the patient underwent a right adrenalectomy. Histopathological analysis confirmed the diagnosis of pheochromocytoma. The postoperative course was uneventful. Pheochromocytomas are most often benign but may be associated with severe cardiovascular complications due to catecholamine excess. Their clinical diagnosis remains challenging due to the lack of specific signs and symptoms. The diagnosis relies on biochemical assays of catecholamine metabolites, supported by functional and anatomical imaging techniques. Surgical excision, preceded by meticulous pharmacologic preparation, remains the cornerstone of treatment. Early diagnosis and appropriate management are essential to prevent potentially life-threatening complications and ensure favorable outcomes.
Keywords: adrenal glands; catecholamine hypersecretion; giant pheochromocytoma; hypertension; scintigraphy.
Copyright © 2025, Chaari et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures



References
-
- The penetrance of paraganglioma and pheochromocytoma in SDHB germline mutation carriers. Rijken JA, Niemeijer ND, Jonker MA, et al. Clin Genet. 2018;93:60–66. - PubMed
-
- Approach to the patient with metastatic pheochromocytoma and paraganglioma. Alkaissi H, Taieb D, Lin FI, Del Rivero J, Wang K, Clifton-Bligh R, Pacak K. J Clin Endocrinol Metab. 2025:0. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials