

Cortical bone mechanics technology signal quality maintains robustness across a range of biometric profiles
- PMID: 40842906
- PMCID: PMC12366785
- DOI: 10.1093/jbmrpl/ziaf116
Cortical bone mechanics technology signal quality maintains robustness across a range of biometric profiles
Abstract
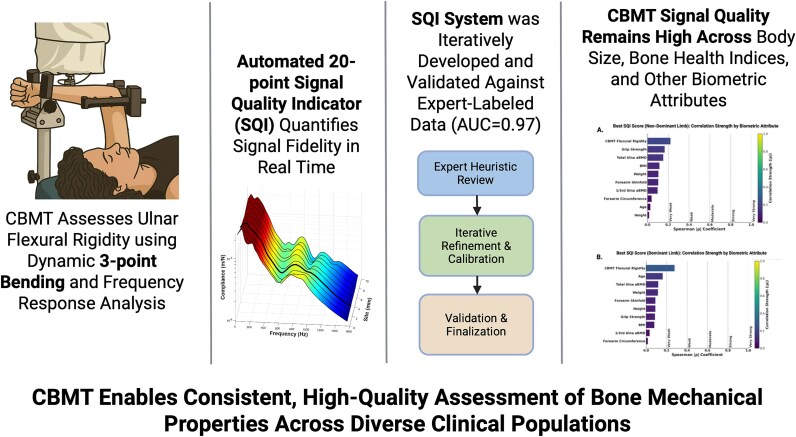
Current methods of diagnosing osteoporosis, such as DXA, have limitations in predicting fracture risk. Cortical bone mechanics technology (CBMT) offers a novel approach by using a three-point bend test with multifrequency vibration analysis to directly measure ulnar bending stiffness and calculate flexural rigidity, a mechanical property highly predictive of whole-bone strength under bending conditions. Cortical bone mechanics technology targets the diaphyseal ulna, a site composed primarily of cortical bone, enhancing its specificity for cortical bone quality. In this study of 388 postmenopausal women, we developed and validated a 20-point signal quality indicator (SQI) scoring system to quantify CBMT signal quality and evaluated its relationship to biometric characteristics. The SQI was developed through expert assessment of representative frequency response function (vibration data) trials and refined over 17 iterations. The final system achieved excellent classification performance (AUC = 0.974; sensitivity, specificity, and accuracy all >97%). A total of 22 740 trials were collected across 758 total arm tests, sampling 10 ulnar sites per arm under three vibration amplitudes. Two expert analysts evaluated signal features associated with high signal quality. The resulting SQI is fully automated and provides real-time feedback. All correlations between SQI scores and biometric attributes were weak or very weak (|ρ| < 0.30). The correlations with body weight (ρ = -0.11), BMI (ρ = -0.12), ulnar BMD (ρ = -0.17), CBMT-derived flexural rigidity (ρ = -0.28), and grip strength (ρ = 0.17) were statistically significant (p < .05) but remained small in magnitude. SQI scores were modestly lower in individuals with higher BMI or flexural rigidity (~2 to 3 points), but values remained in the acceptable-to-good range. This study introduces a robust, automated CBMT signal quality metric and demonstrates that its performance remains stable across a broad range of biometric profiles, supporting its application in both clinical and research settings.
Keywords: BMD; bone strength; cortical bone mechanics technology (CBMT); fracture; mechanical response tissue analysis (MRTA); osteoporosis.
© The Author(s) 2025. Published by Oxford University Press on behalf of the American Society for Bone and Mineral Research.
Conflict of interest statement
B.C.C. is a co-founder with equity in OsteoDx, Inc. A.D. and M.S. are employees of OsteoDx Inc. M.R. has served as a consultant to OsteoDx Inc. T.S. serves as a consultant to OsteoDx, Inc. and represents an investor in the company.
Figures







References
-
- NIH . Osteoporosis, Health and Human Services. Bethesda, MD: National Institutes of Health; 2018: No. 18-AR-8004.
-
- Hansen D et al. Medicare cost of osteoporotic fractures: the clinical and cost burden of an important consequence of osteoporosis. Commissioned by the National Osteoporosis Foundation. 2019;
LinkOut - more resources
Full Text Sources
