

Volumetric Assessment of Perimesencephalic Subarachnoid Hemorrhage
- PMID: 40844796
- PMCID: PMC12450190
- DOI: 10.1007/s40120-025-00813-y
Volumetric Assessment of Perimesencephalic Subarachnoid Hemorrhage
Abstract
Introduction: Perimesencephalic subarachnoid hemorrhage (pmSAH) is a rare, typically benign subtype of non-aneurysmal subarachnoid hemorrhage (SAH). While the majority of patients demonstrate a positive recovery trajectory, a subset of patients experiences complications, including vasospasm, hydrocephalus, or delayed cerebral ischemia (DCI). Reliable imaging markers for risk stratification are lacking. This study evaluates whether volumetric CT-based biomarkers-validated in aneurysmal SAH (aSAH)-are also predictive for pmSAH.
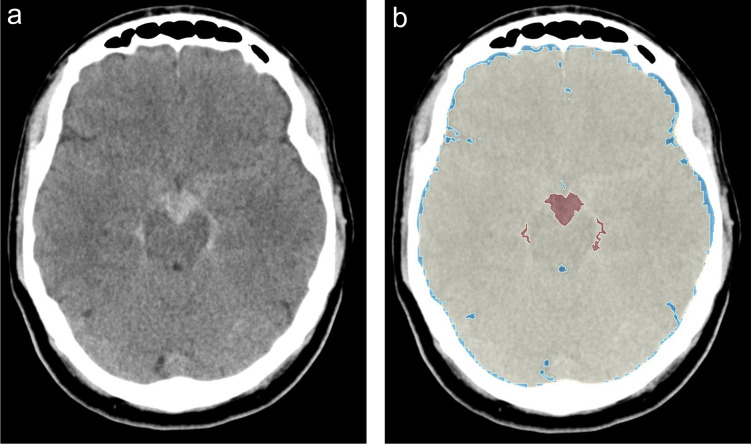
Methods: In this retrospective single-center study, 72 patients with confirmed pmSAH between 2011 and 2024 were analyzed. The automated volumetric segmentation was performed using 3D Slicer and TotalSegmentator to quantify intracranial volume (ICV), brain volume (BV), cerebrospinal fluid (CSF), and selective sulcal volume (SSV). The associations between volumetric parameters and clinical presentation, complications, and functional outcome (Glasgow Outcome Scale, GOS) were assessed using non-parametric statistics and Spearman correlation.
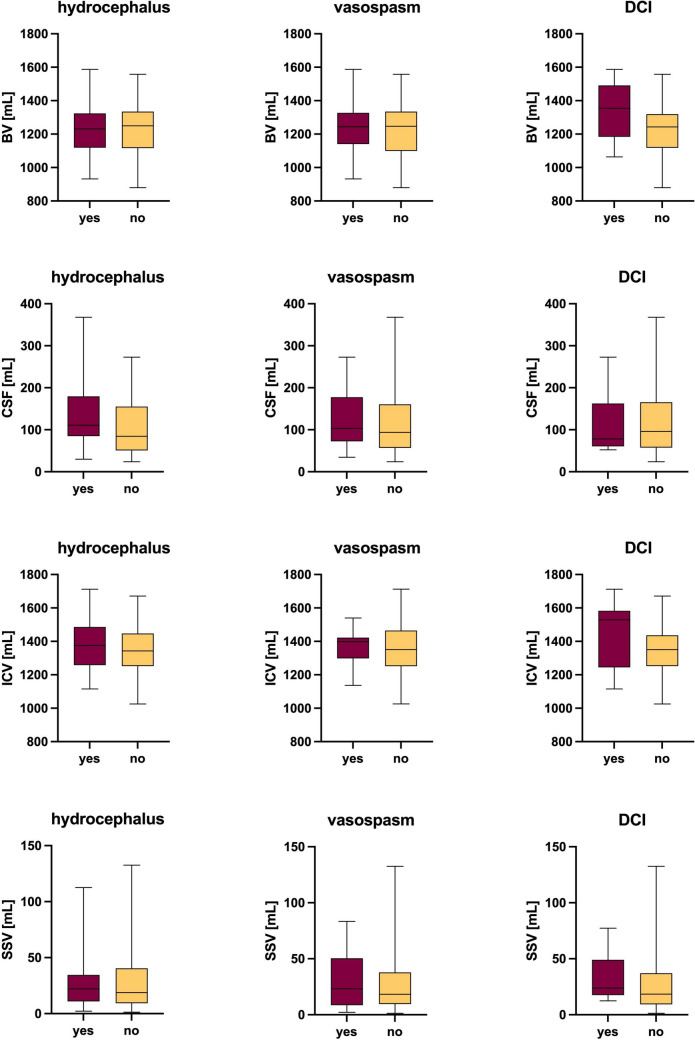
Results: The median intracranial volume was 1352.7 mL, brain volume 1247.3 mL, cerebrospinal fluid volume 95.9 mL, and selective sulcal volume 19.4 mL. Vomiting at presentation was associated with higher CSF and SSV values (p = 0.04 and p = 0.005, respectively), but no significant volumetric differences were found regarding other symptoms or complications (vasospasm, hydrocephalus, DCI). GOS scores were uniformly high (median = 5), and none of the volumetric markers significantly correlated with outcome or complication rate (all p > 0.05).
Conclusion: In contrast to aSAH, volumetric CT biomarkers such as ICV, BV, CSF, and SSV do not offer predictive value in patients with pmSAH. Risk stratification should continue to rely on initial hemorrhage pattern and volume, clinical monitoring, and individualized assessment rather than other volumetric parameters.
Keywords: Delayed cerebral ischemia; Hydrocephalus; Perimesencephalic subarachnoid hemorrhage; Subarachnoid hemorrhage; Vasospasm; Volumetric analysis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: Emily Hoffmann, Hermann Krähling, Moritz Kleinevoss, Công Duy Bùi, Ziad Maksoud, Markus Holling, Michael Köhler, Tobias D. Faizy, Christian Paul Stracke, Burak Han Akkurt declare that they have no conflict of interest. Ethical Approval: The study was conducted in accordance with the tenets of the Declaration of Helsinki (as revised in 2013), and the study was approved by the local ethics committee of the University of Münster (2023-415-f-S). Informed consent was not obtained from patients due to the retrospective nature of this study.
Figures
References
-
- Alrohimi A, Davison MA, Pandhi A, et al. Aneurysmal Versus “Benign” Perimesencephalic Subarachnoid Hemorrhage. Stroke. 2024;4:e001166. 10.1161/SVIN.123.001166. - DOI
LinkOut - more resources
Full Text Sources
